

IL-6-based mortality prediction model for COVID-19: Validation and update in multicenter and second wave cohorts
- PMID: 33662370
- PMCID: PMC7919507
- DOI: 10.1016/j.jaci.2021.02.021
IL-6-based mortality prediction model for COVID-19: Validation and update in multicenter and second wave cohorts
Abstract
Background: Coronavirus disease 2019 (COVID-19) is a highly variable condition. Validated tools to assist in the early detection of patients at high risk of mortality can help guide medical decisions.
Objective: We sought to validate externally, as well as in patients from the second pandemic wave in Europe, our previously developed mortality prediction model for hospitalized COVID-19 patients.
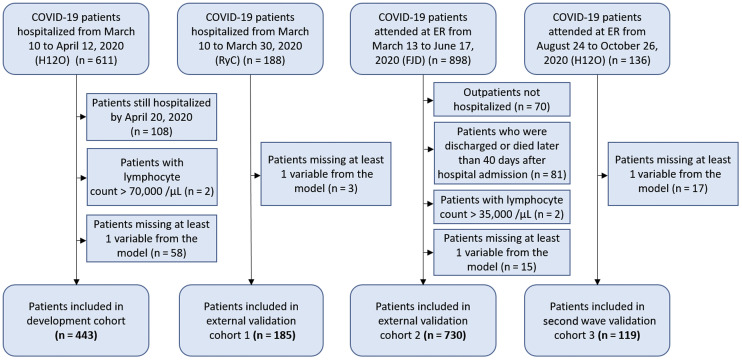
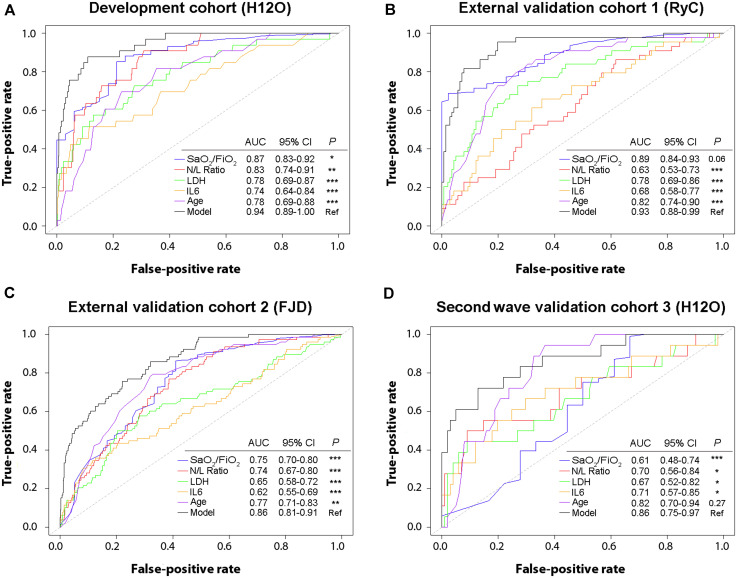
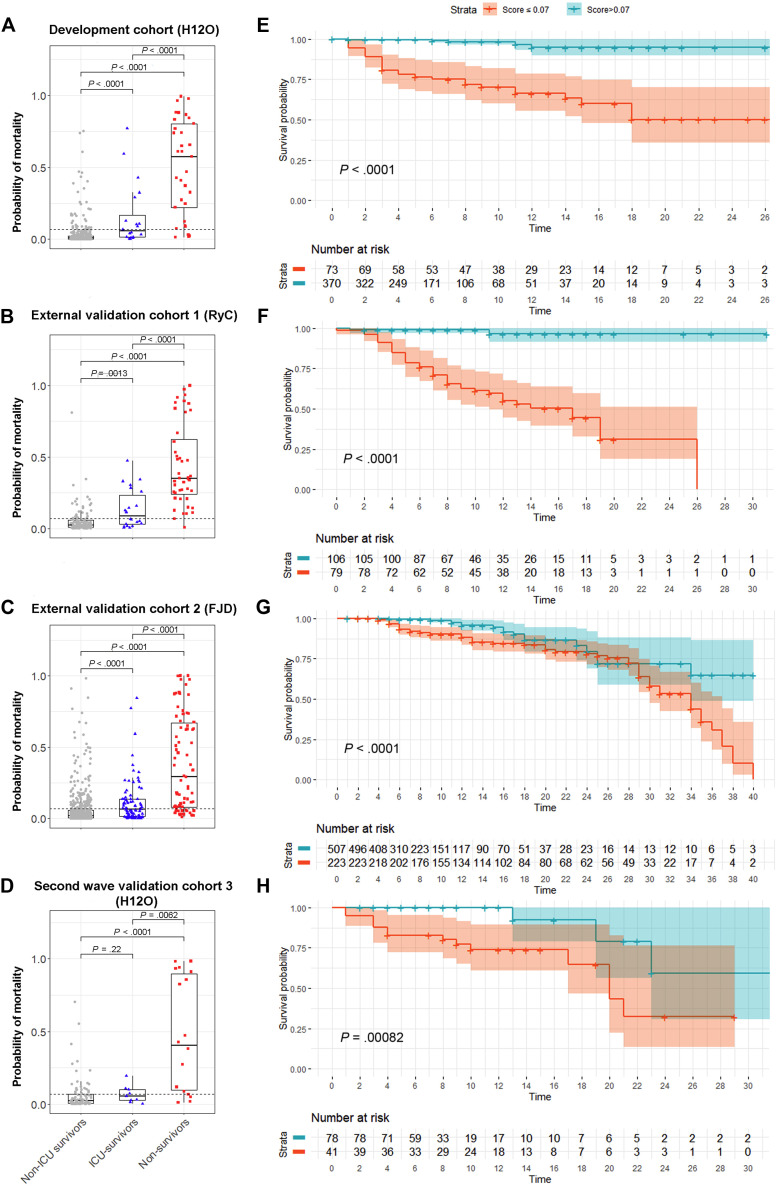
Methods: Three validation cohorts were generated: 2 external with 185 and 730 patients from the first wave and 1 internal with 119 patients from the second wave. The probability of death was calculated for all subjects using our prediction model, which includes peripheral blood oxygen saturation/fraction of inspired oxygen ratio, neutrophil-to-lymphocyte ratio, lactate dehydrogenase, IL-6, and age. Discrimination and calibration were evaluated in the validation cohorts. The prediction model was updated by reestimating individual risk factor effects in the overall cohort (N = 1477).
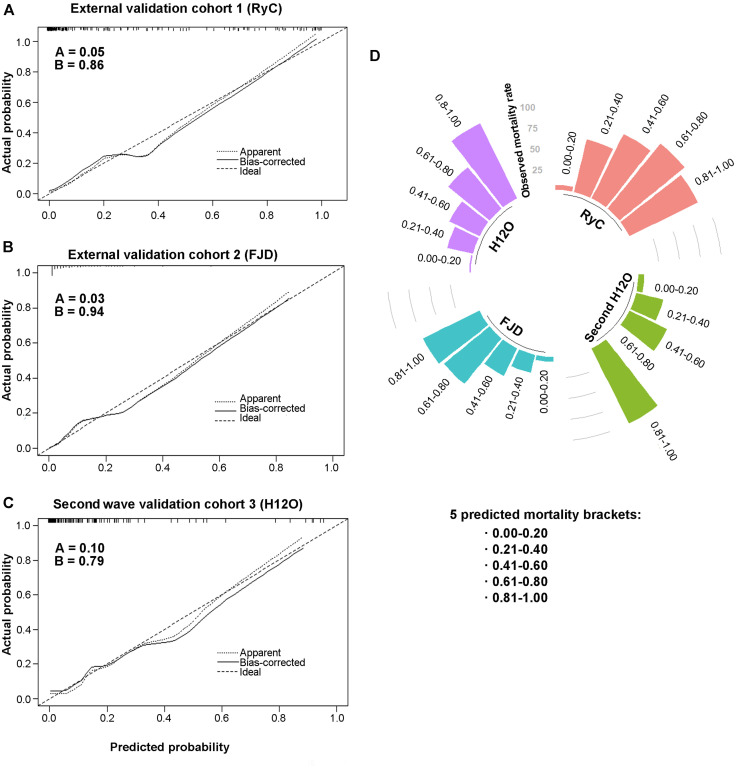
Results: The mortality prediction model showed good performance in the external validation cohorts 1 and 2, and in the second wave validation cohort 3 (area under the receiver-operating characteristic curve, 0.94, 0.86, and 0.86, respectively), with excellent calibration (calibration slope, 0.86, 0.94, and 0.79; intercept, 0.05, 0.03, and 0.10, respectively). The updated model accurately predicted mortality in the overall cohort (area under the receiver-operating characteristic curve, 0.91), which included patients from both the first and second COVID-19 waves. The updated model was also useful to predict fatal outcome in patients without respiratory distress at the time of evaluation.
Conclusions: This is the first COVID-19 mortality prediction model validated in patients from the first and second pandemic waves. The COR+12 online calculator is freely available to facilitate its implementation (https://utrero-rico.shinyapps.io/COR12_Score/).
Keywords: COVID-19; IL-6; external validation; mortality risk; predictive model; second wave.
Copyright © 2021 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Coronavirus Resource Center https://coronavirus.jhu.edu/ Available at:
-
- World Health Organization https://who.maps.arcgis.com/apps/opsdashboard/index.html#/ead3c647565448... Available at:
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
