

Activation of astroglial CB1R mediates cerebral ischemic tolerance induced by electroacupuncture
- PMID: 33663269
- PMCID: PMC8393297
- DOI: 10.1177/0271678X21994395
Activation of astroglial CB1R mediates cerebral ischemic tolerance induced by electroacupuncture
Abstract
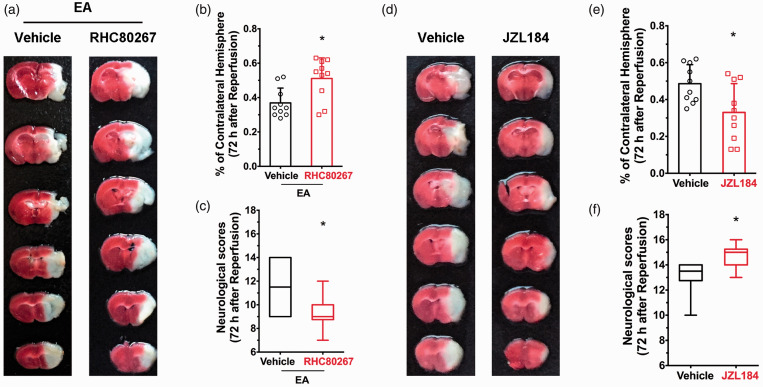
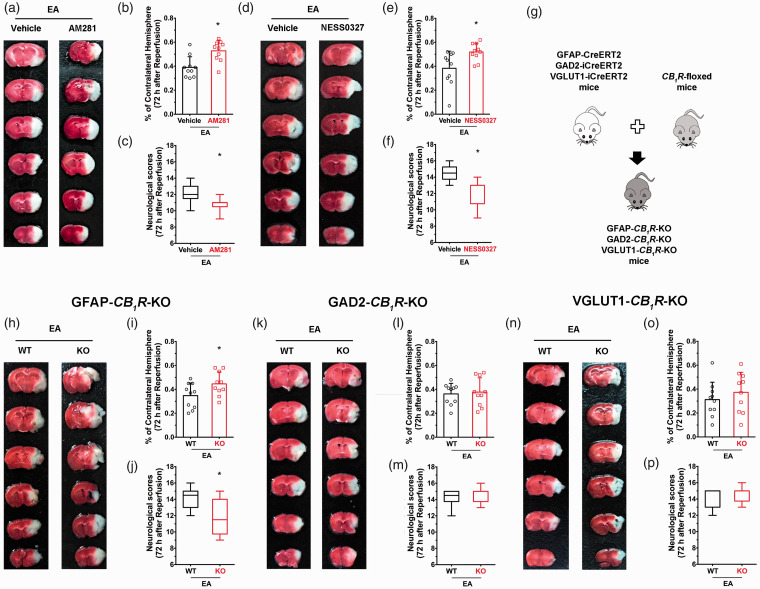
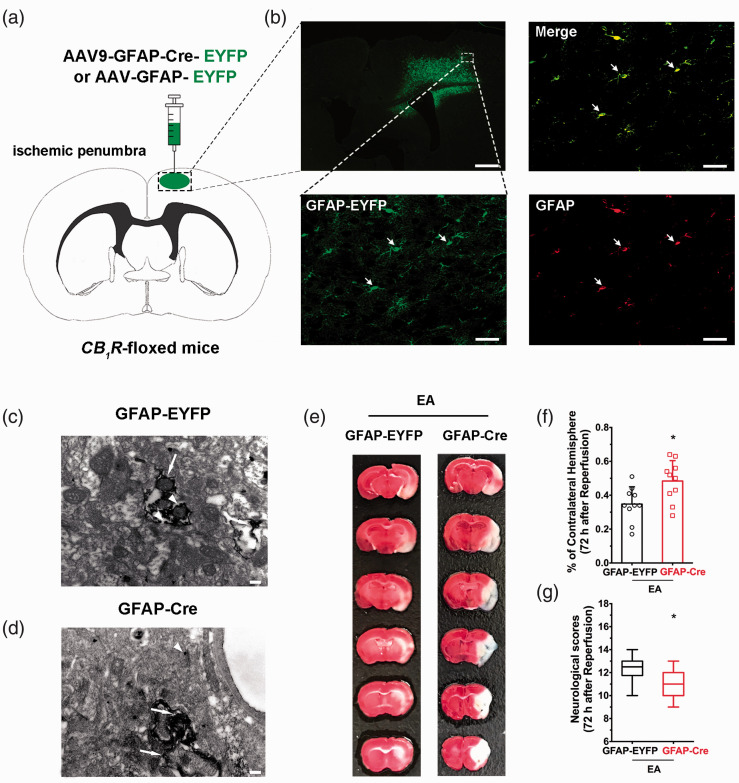
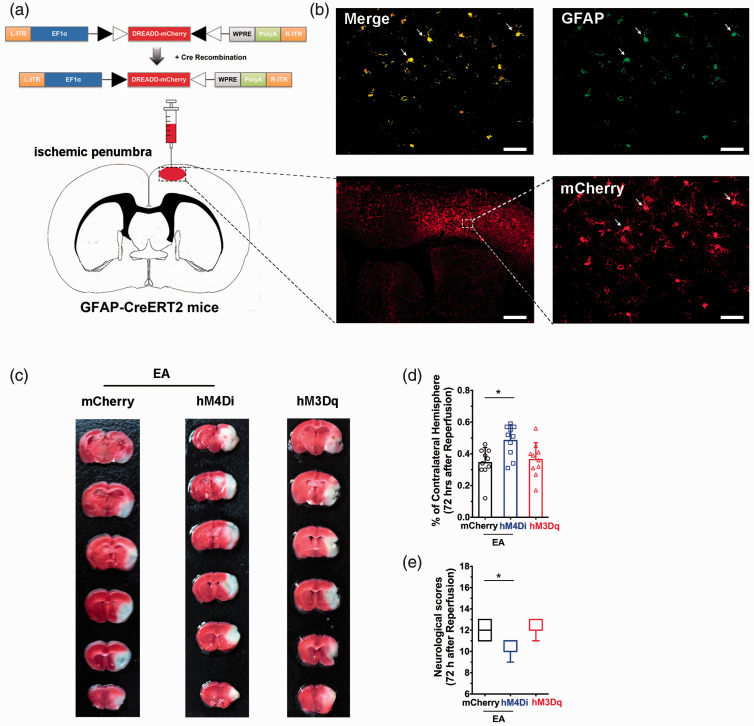
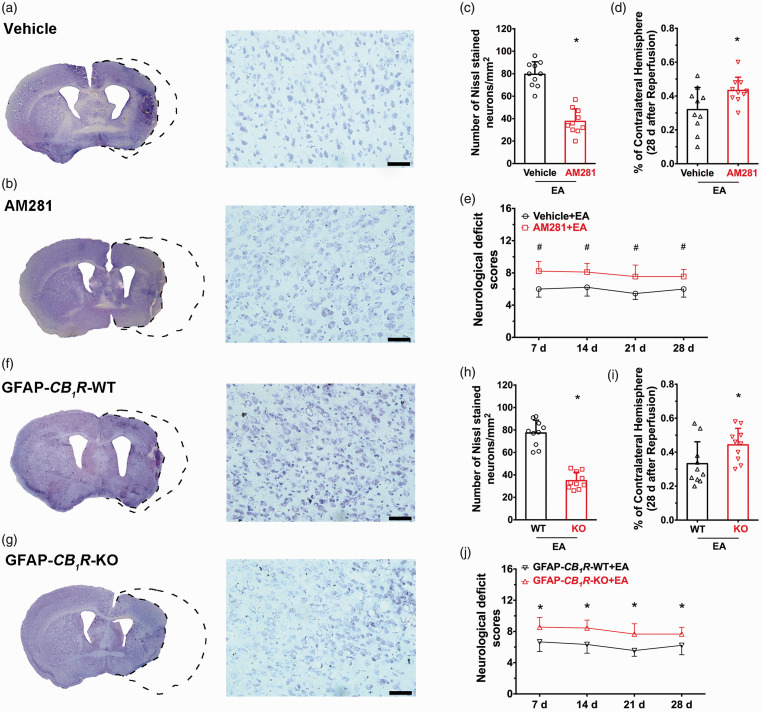
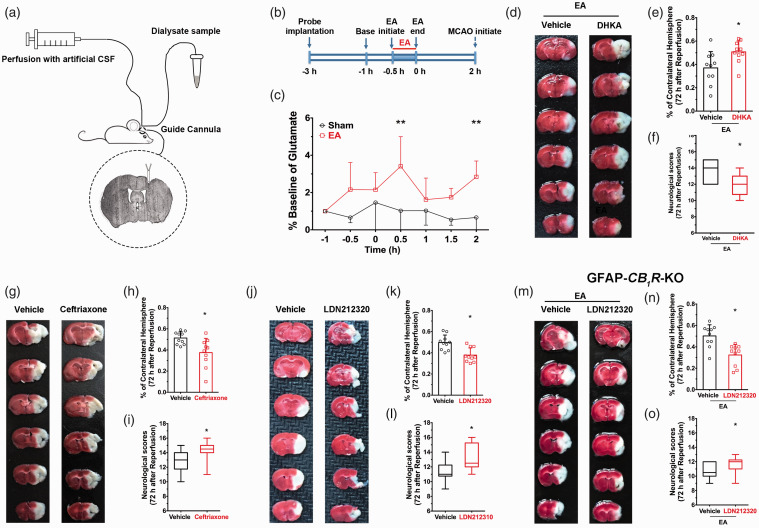
There are no effective treatments for stroke. The activation of endogenous protective mechanisms is a promising therapeutic approach, which evokes the intrinsic ability of the brain to protect itself. Accumulated evidence strongly suggests that electroacupuncture (EA) pretreatment induces rapid tolerance to cerebral ischemia. With regard to mechanisms underlying ischemic tolerance induced by EA, many molecules and signaling pathways are involved, such as the endocannabinoid system, although the exact mechanisms have not been fully elucidated. In the current study, we employed mutant mice, neuropharmacology, microdialysis, and virus transfection techniques in a middle cerebral artery occlusion (MCAO) model to explore the cell-specific and brain region-specific mechanisms of EA-induced neuroprotection. EA pretreatment resulted in increased ambient endocannabinoid (eCB) levels and subsequent activation of ischemic penumbral astroglial cannabinoid type 1 receptors (CB1R) which led to moderate upregulation of extracellular glutamate that protected neurons from cerebral ischemic injury. These findings provide a novel cellular mechanism of EA and a potential therapeutic target for ischemic stroke.
Keywords: Astrocyte; CB1R; electroacupuncture; pretreatment; stroke.
Conflict of interest statement
Figures
Similar articles
-
Activation of STAT3 is involved in neuroprotection by electroacupuncture pretreatment via cannabinoid CB1 receptors in rats.Brain Res. 2013 Sep 5;1529:154-64. doi: 10.1016/j.brainres.2013.07.006. Epub 2013 Jul 20. Brain Res. 2013. PMID: 23880371
-
Mn-SOD Upregulation by Electroacupuncture Attenuates Ischemic Oxidative Damage via CB1R-Mediated STAT3 Phosphorylation.Mol Neurobiol. 2016 Jan;53(1):331-343. doi: 10.1007/s12035-014-8971-7. Epub 2014 Nov 29. Mol Neurobiol. 2016. PMID: 25432886
-
Activation of epsilon protein kinase C-mediated anti-apoptosis is involved in rapid tolerance induced by electroacupuncture pretreatment through cannabinoid receptor type 1.Stroke. 2011 Feb;42(2):389-96. doi: 10.1161/STROKEAHA.110.597336. Epub 2010 Dec 23. Stroke. 2011. PMID: 21183751
-
Stimulated CB1 Cannabinoid Receptor Inducing Ischemic Tolerance and Protecting Neuron from Cerebral Ischemia.Cent Nerv Syst Agents Med Chem. 2017;17(2):141-150. doi: 10.2174/1871524916666160504104624. Cent Nerv Syst Agents Med Chem. 2017. PMID: 27142423 Review.
-
CB1R-dependent regulation of astrocyte physiology and astrocyte-neuron interactions.Neuropharmacology. 2021 Sep 1;195:108678. doi: 10.1016/j.neuropharm.2021.108678. Epub 2021 Jun 19. Neuropharmacology. 2021. PMID: 34157362 Review.
Cited by
-
Preserving stroke penumbra by targeting lipid signalling.J Cereb Blood Flow Metab. 2023 Jan;43(1):167-169. doi: 10.1177/0271678X221121853. Epub 2022 Aug 23. J Cereb Blood Flow Metab. 2023. PMID: 35999812 Free PMC article.
-
The Role of Astrocytes in Poststroke Rehabilitation.Brain Behav. 2025 Jun;15(6):e70551. doi: 10.1002/brb3.70551. Brain Behav. 2025. PMID: 40462588 Free PMC article. Review.
-
Electroacupuncture Promotes the Generation of Intestinal Treg Cells After Ischemic Stroke by Foxp3 Acetylation Regulation.Mol Neurobiol. 2025 Mar;62(3):3697-3711. doi: 10.1007/s12035-024-04500-1. Epub 2024 Sep 25. Mol Neurobiol. 2025. PMID: 39322831
-
Potential mechanisms of acupuncture in enhancing cerebral perfusion of ischemic stroke.Front Neurol. 2022 Oct 28;13:1030747. doi: 10.3389/fneur.2022.1030747. eCollection 2022. Front Neurol. 2022. PMID: 36388196 Free PMC article. Review.
-
The effect of cannabinoid type Ⅱ receptor on the excitability of substantia nigra dopaminergic neurons.Front Pharmacol. 2025 Feb 14;16:1522210. doi: 10.3389/fphar.2025.1522210. eCollection 2025. Front Pharmacol. 2025. PMID: 40028168 Free PMC article.
References
-
- Johnston SC, Mendis S, Mathers CD.Global variation in stroke burden and mortality: estimates from monitoring, surveillance, and modelling. Lancet Neurol 2009; 8: 345–354. - PubMed
-
- Hoyert DL, Xu J.Deaths: preliminary data for 2011. Natl Vital Stat Rep 2012; 61: 1–51. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, et al.. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation 2016; 133: e38–e360. - PubMed
-
- Chen G, Leak RK, Sun Q, et al.. Neurobiology of stroke: research progress and perspectives. Prog Neurobiol 2018; 163-164: 1–4. 4. - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, et al.. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2018; 49: e46–e110. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
