

Histological diagnostic criterion for chronic endometritis based on the clinical outcome
- PMID: 33663485
- PMCID: PMC7934457
- DOI: 10.1186/s12905-021-01239-y
Histological diagnostic criterion for chronic endometritis based on the clinical outcome
Abstract
Background: The diagnostic criteria of chronic endometritis remain controversial in the treatment for infertile patients.
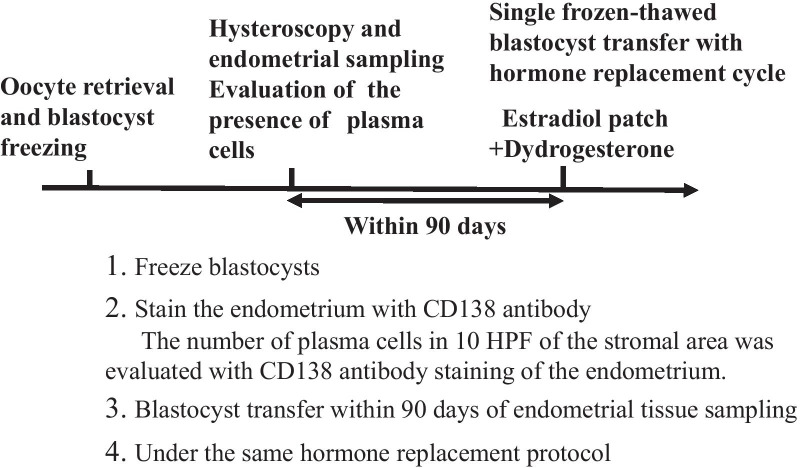
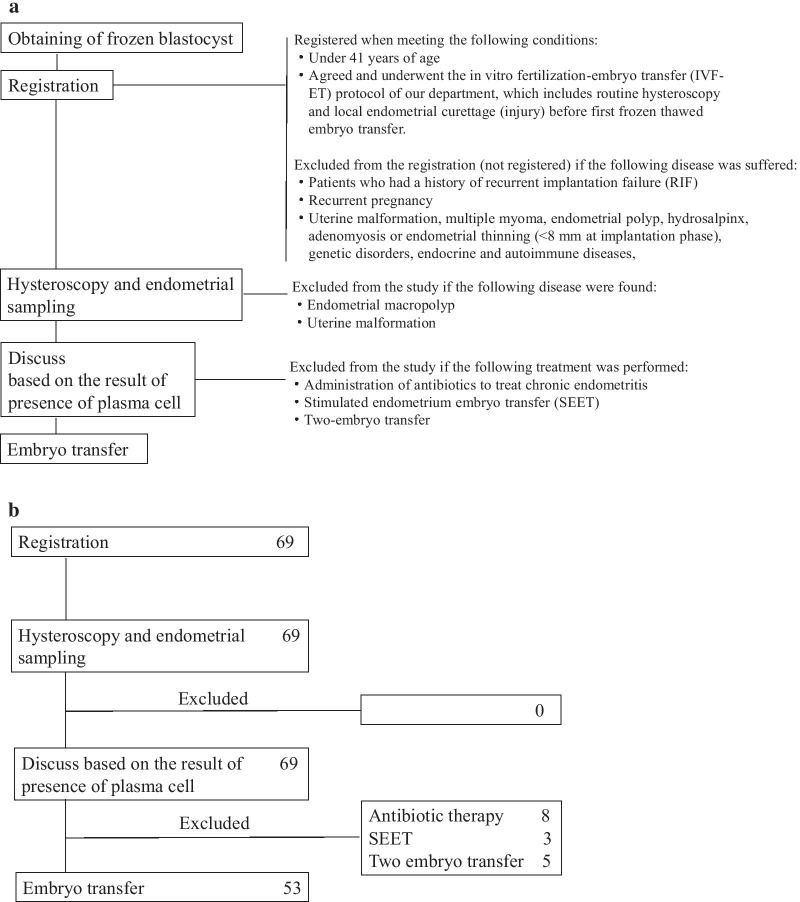
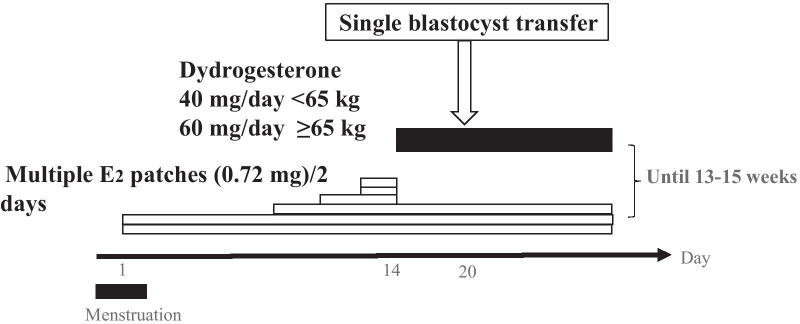
Methods: A prospective observational study was conducted in a single university from June 2014 to September 2017. Patients who underwent single frozen-thawed blastocyst transfer with a hormone replacement cycle after histological examination for the presence of chronic endometritis were enrolled. Four criteria were used to define chronic endometritis according to the number of plasma cells in the same group of patients: 1 or more (≥ 1) plasma cells, 2 or more (≥ 2), 3 or more (≥ 3), or 5 or more (≥ 5) in 10 high-power fields. Pregnancy rates, live birth rates, and miscarriage rates of the non-chronic endometritis and the chronic endometritis groups defined with each criterion were calculated. A logistic regression analysis was performed for live births using eight explanatory variables (seven infertility factors and chronic endometritis). A receiver operating characteristic curve was drawn and the optimal cut-off value was calculated.
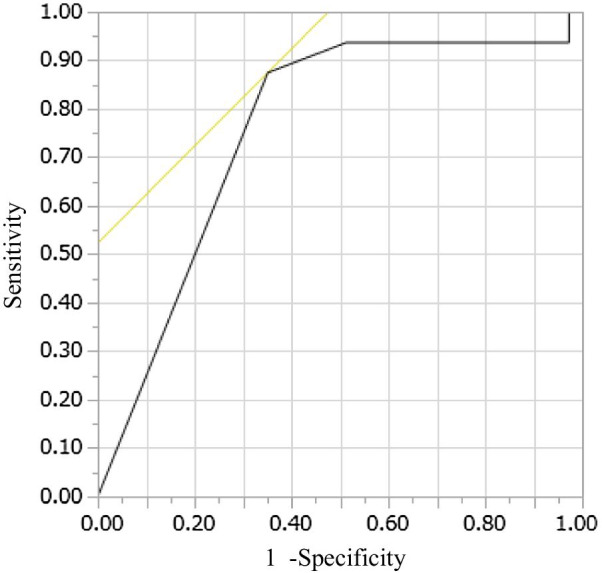
Results: A total of 69 patients were registered and 53 patients were finally analyzed after exclusion. When the diagnostic criterion was designated as the presence of ≥ 1 plasma cell in the endometrial stroma per 10 high-power fields, the pregnancy rate, live birth rate, and miscarriage rate were 63.0% vs. 30.8%, 51.9% vs. 7.7%, and 17.7% vs. 75% in the non-chronic and chronic endometritis groups, respectively. This criterion resulted in the highest pregnancy and live birth rates among the non-chronic endometritis and the smallest P values for the pregnancy rates, live birth rates, and miscarriage rates between the non-chronic and chronic endometritis groups. In the logistic regression analysis, chronic endometritis was an explanatory variable negatively affecting the objective variable of live birth only when chronic endometritis was diagnosed with ≥ 1 or ≥ 2 plasma cells per 10 high-power fields. The optimal cut-off value was obtained when one or more plasma cells were found in 10 high-power fields (sensitivity 87.5%, specificity 64.9%).
Conclusions: Chronic endometritis should be diagnosed as the presence of ≥ 1 plasma cells in 10 high-power fields. According to this diagnostic criterion, chronic endometritis adversely affected the pregnancy rate and the live birth rate.
Keywords: Chronic endometritis; Diagnostic criterion; Infertility; Plasma cell.
Conflict of interest statement
No author has any conflict of interest to disclose.
Figures
Similar articles
-
The effects of chronic endometritis on the pregnancy outcomes.Am J Reprod Immunol. 2021 Mar;85(3):e13357. doi: 10.1111/aji.13357. Epub 2020 Oct 23. Am J Reprod Immunol. 2021. PMID: 33020952
-
[The effect of chronic endometritis on the clinical outcomes of patients with failure of first embryo transfer].Zhonghua Yi Xue Za Zhi. 2023 Jul 25;103(28):2157-2162. doi: 10.3760/cma.j.cn112137-20221127-02517. Zhonghua Yi Xue Za Zhi. 2023. PMID: 37482727 Chinese.
-
Impact of oral antibiotic treatment for chronic endometritis on pregnancy outcomes in the following frozen-thawed embryo transfer cycles of infertile women: a cohort study of 640 embryo transfer cycles.Fertil Steril. 2021 Aug;116(2):413-421. doi: 10.1016/j.fertnstert.2021.03.036. Epub 2021 Apr 26. Fertil Steril. 2021. PMID: 33926717
-
Variation of diagnostic criteria in women with chronic endometritis and its effect on reproductive outcomes: A systematic review and meta-analysis.J Reprod Immunol. 2020 Aug;140:103146. doi: 10.1016/j.jri.2020.103146. Epub 2020 May 19. J Reprod Immunol. 2020. PMID: 32442825
-
Effects of chronic endometritis therapy on in vitro fertilization outcome in women with repeated implantation failure: a systematic review and meta-analysis.Fertil Steril. 2018 Jul 1;110(1):103-112.e1. doi: 10.1016/j.fertnstert.2018.03.017. Epub 2018 Jun 13. Fertil Steril. 2018. PMID: 29908776
Cited by
-
Chronic endometritis and the endometrial microbiota: implications for reproductive success in patients with recurrent implantation failure.Ann Clin Microbiol Antimicrob. 2024 May 30;23(1):49. doi: 10.1186/s12941-024-00710-6. Ann Clin Microbiol Antimicrob. 2024. PMID: 38816832 Free PMC article.
-
Alterations in Implantation Genes and Dendritic Cells in Endometrial Samples After Antibiotic Treatment.J Clin Med. 2025 Jan 27;14(3):834. doi: 10.3390/jcm14030834. J Clin Med. 2025. PMID: 39941505 Free PMC article.
-
Prevalence of chronic endometritis in infertile women undergoing hysteroscopy and its association with intrauterine abnormalities: A Cross-Sectional study.JBRA Assist Reprod. 2024 Aug 26;28(3):430-434. doi: 10.5935/1518-0557.20240011. JBRA Assist Reprod. 2024. PMID: 38546120 Free PMC article.
-
Histopathological evaluation of cesarean scar defect in women with cesarean scar syndrome.Reprod Med Biol. 2021 Dec 21;21(1):e12431. doi: 10.1002/rmb2.12431. eCollection 2022 Jan-Dec. Reprod Med Biol. 2021. PMID: 35386374 Free PMC article.
-
Antibiotics combined with vaginal probiotics in the embryo transfer cycle of infertile patients with chronic endometritis.Front Cell Infect Microbiol. 2024 Nov 28;14:1494931. doi: 10.3389/fcimb.2024.1494931. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39669276 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
