

Standard of care versus new-wave corticosteroids in the treatment of Duchenne muscular dystrophy: Can we do better?
- PMID: 33663533
- PMCID: PMC7934375
- DOI: 10.1186/s13023-021-01758-9
Standard of care versus new-wave corticosteroids in the treatment of Duchenne muscular dystrophy: Can we do better?
Abstract
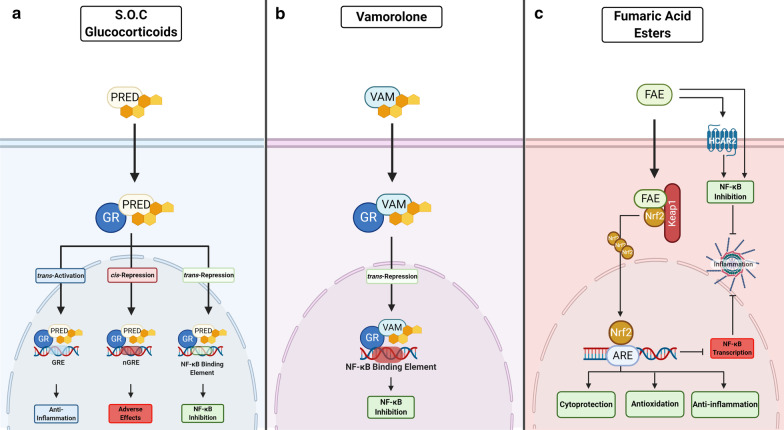
Background: Pharmacological corticosteroid therapy is the standard of care in Duchenne Muscular Dystrophy (DMD) that aims to control symptoms and slow disease progression through potent anti-inflammatory action. However, a major concern is the significant adverse effects associated with long term-use. MAIN: This review discusses the pros and cons of standard of care treatment for DMD and compares it to novel data generated with the new-wave dissociative corticosteroid, vamorolone. The current status of experimental anti-inflammatory pharmaceuticals is also reviewed, with insights regarding alternative drugs that could provide therapeutic advantage.
Conclusions: Although novel dissociative steroids may be superior substitutes to corticosteroids, other potential therapeutics should be explored. Repurposing or developing novel pharmacological therapies capable of addressing the many pathogenic features of DMD in addition to anti-inflammation could elicit greater therapeutic advantages.
Keywords: Anti-inflammation; Anti-inflammatory drugs; Corticosteroids; Duchenne muscular dystrophy; Standard of care.
Conflict of interest statement
E.R. and N.G. are consultants to Santhera Pharmaceuticals. E.R. is a consultant to Epirium Bio. D.F. is a principal investigator for studies on spinal muscular atrophy sponsored by Hofmann-La Roche Ltd. The other authors have no interests to declare.
Figures
References
-
- Nicolas A, Lucchetti-Miganeh C, Yaou RB, Kaplan J-C, Chelly J, Leturcq F, Barloy-Hubler F, Le Rumeur E. Assessment of the structural and functional impact of in-frame mutations of the DMD gene, using the tools included in the eDystrophin online database. Orphanet J Rare Dis. 2012;7:45. doi: 10.1186/1750-1172-7-45. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
