

Closed-Loop Electronic Referral From Primary Care Clinics to a State Tobacco Cessation Quitline: Effects Using Real-World Implementation Training
- PMID: 33663698
- PMCID: PMC7939019
- DOI: 10.1016/j.amepre.2019.12.026
Closed-Loop Electronic Referral From Primary Care Clinics to a State Tobacco Cessation Quitline: Effects Using Real-World Implementation Training
Abstract
Introduction: Patients who use tobacco are too rarely connected with tobacco use treatment during healthcare visits. Electronic health record enhancements may increase such referrals in primary care settings. This project used the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework to assess the implementation of a healthcare system change carried out in an externally valid manner (executed by the healthcare system).
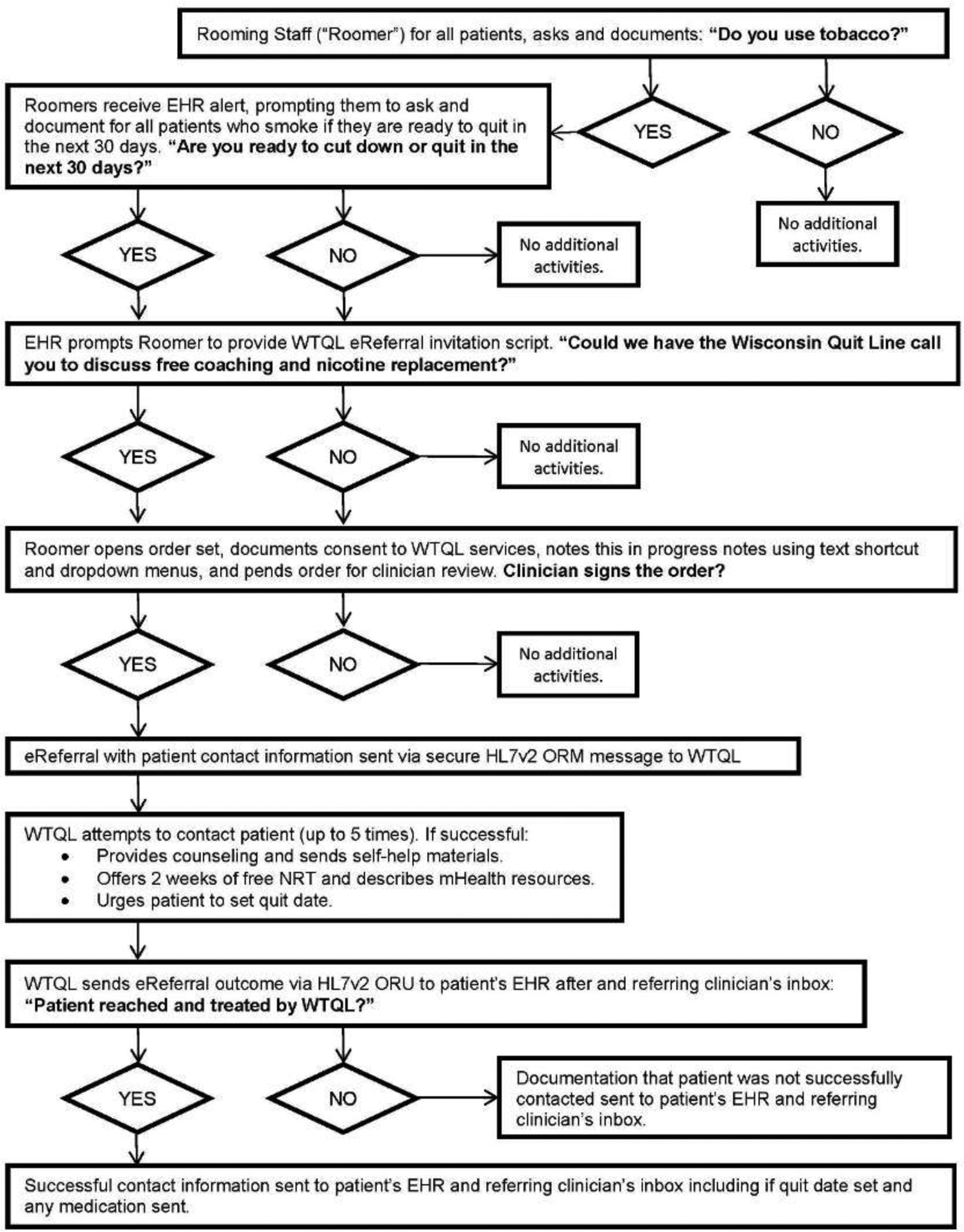
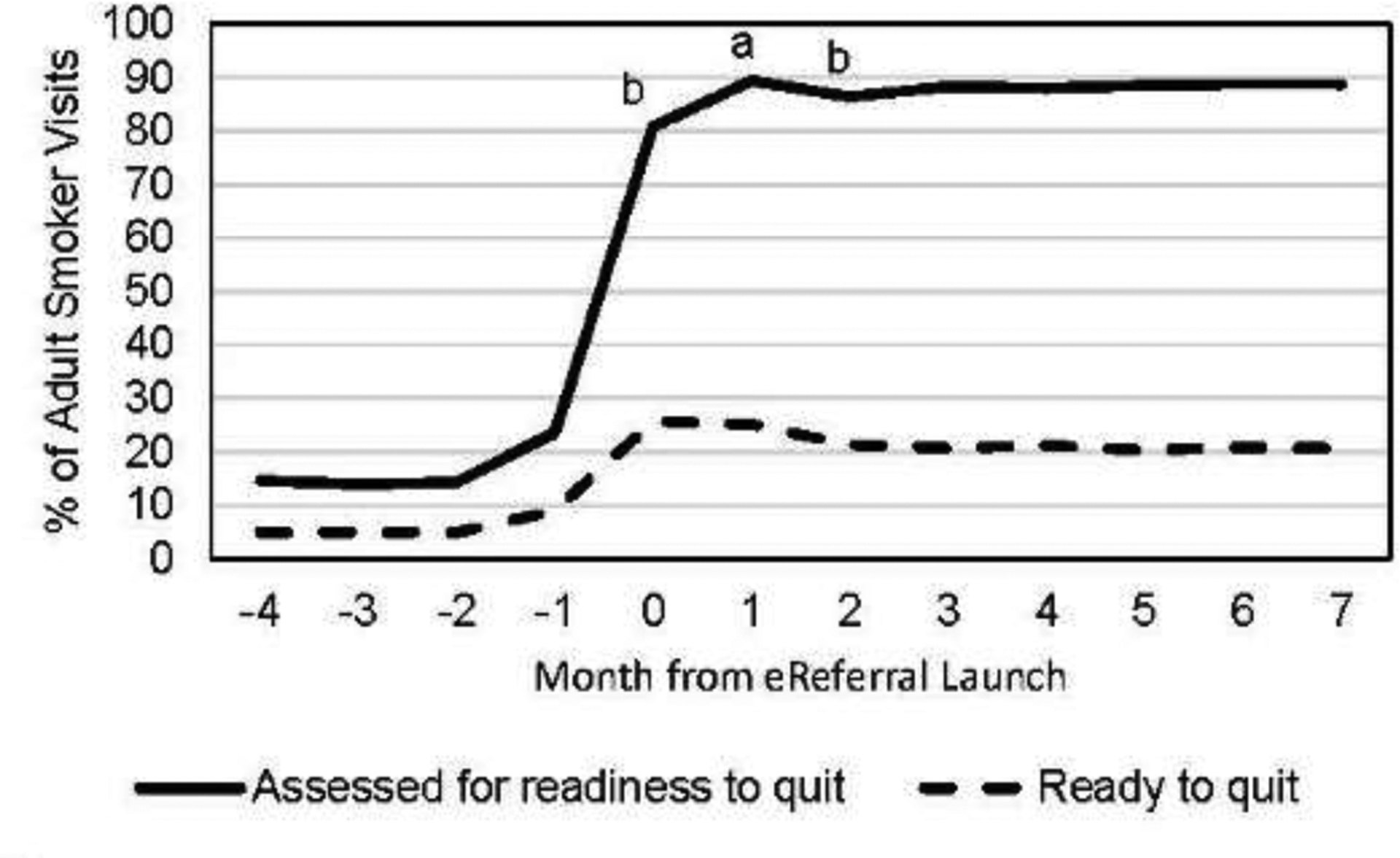
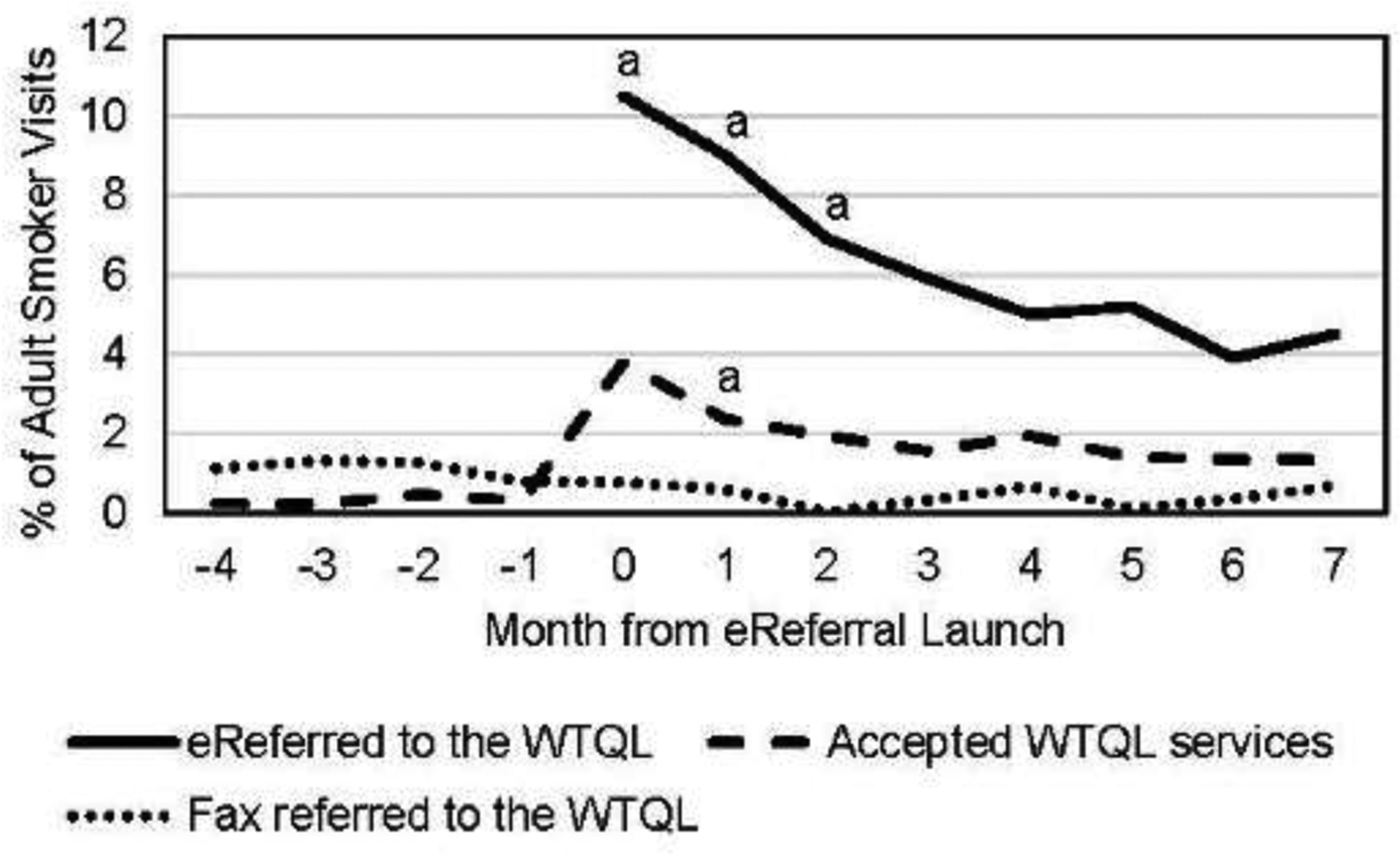
Methods: The healthcare system used their standard, computer-based training approach to implement the electronic health record and clinic workflow changes for electronic referral in 30 primary care clinics that previously used faxed quitline referral. Electronic health record data captured rates of assessment of readiness to quit and quitline referral 4 months before implementation and 8 months (May-December 2017) after implementation. Data, analyzed from October 2018 to June 2019, also reflected intervention reach, adoption, and maintenance.
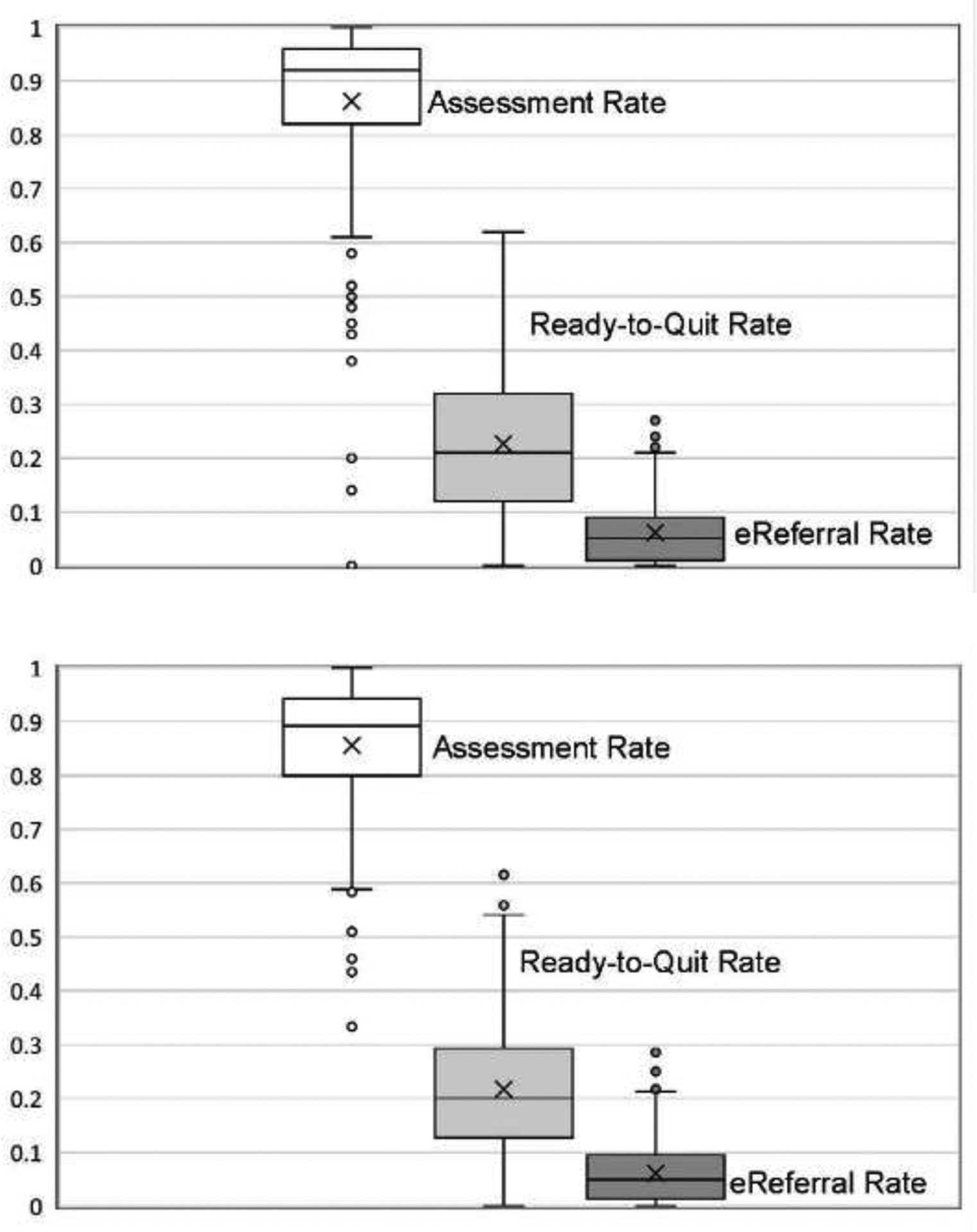
Results: For reach and effectiveness, from before to after implementation for electronic referral, among adult patients who smoked, assessment of readiness to quit increased from 24.8% (2,126 of 8,569) to 93.2% (11,163 of 11,977), quitline referrals increased from 1.7% (143 of 8,569) to 11.3% (1,351 of 11,977), and 3.6% were connected with the quitline after implementation. For representativeness of reach, electronic referral rates were especially high for women, African Americans, and Medicaid patients. For adoption, 52.6% of staff who roomed at least 1 patient who smoked referred to the quitline. For maintenance, electronic referral rates fell by approximately 60% over 8 months but remained higher than pre-implementation rates.
Conclusions: Real-world implementation of an electronic health record-based electronic referral system markedly increased readiness to quit assessment and quitline referral rates in primary care patients. Future research should focus on implementation methods that produce more consistent implementation and better maintenance of electronic referral.
Copyright © 2020 American Journal of Preventive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Fiore MC, Jaen CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Rockville, MD: HHS, U.S. Public Health Service; 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
