

Automation of surgical skill assessment using a three-stage machine learning algorithm
- PMID: 33664317
- PMCID: PMC7933408
- DOI: 10.1038/s41598-021-84295-6
Automation of surgical skill assessment using a three-stage machine learning algorithm
Erratum in
-
Author Correction: Automation of surgical skill assessment using a three-stage machine learning algorithm.Sci Rep. 2021 Apr 20;11(1):8933. doi: 10.1038/s41598-021-88175-x. Sci Rep. 2021. PMID: 33879815 Free PMC article. No abstract available.
Abstract
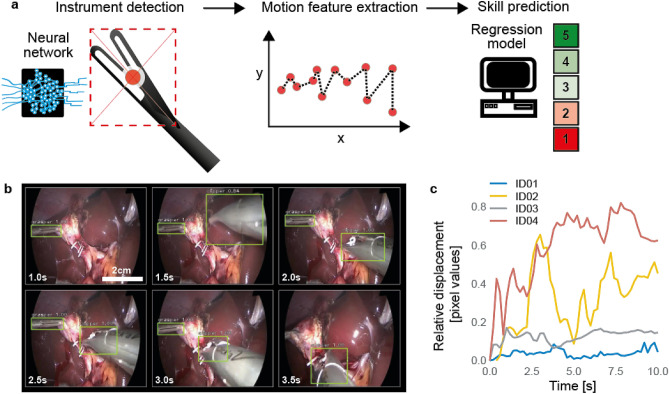
Surgical skills are associated with clinical outcomes. To improve surgical skills and thereby reduce adverse outcomes, continuous surgical training and feedback is required. Currently, assessment of surgical skills is a manual and time-consuming process which is prone to subjective interpretation. This study aims to automate surgical skill assessment in laparoscopic cholecystectomy videos using machine learning algorithms. To address this, a three-stage machine learning method is proposed: first, a Convolutional Neural Network was trained to identify and localize surgical instruments. Second, motion features were extracted from the detected instrument localizations throughout time. Third, a linear regression model was trained based on the extracted motion features to predict surgical skills. This three-stage modeling approach achieved an accuracy of 87 ± 0.2% in distinguishing good versus poor surgical skill. While the technique cannot reliably quantify the degree of surgical skill yet it represents an important advance towards automation of surgical skill assessment.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
