

Transcriptional mediators of treatment resistance in lethal prostate cancer
- PMID: 33664492
- PMCID: PMC7960507
- DOI: 10.1038/s41591-021-01244-6
Transcriptional mediators of treatment resistance in lethal prostate cancer
Abstract
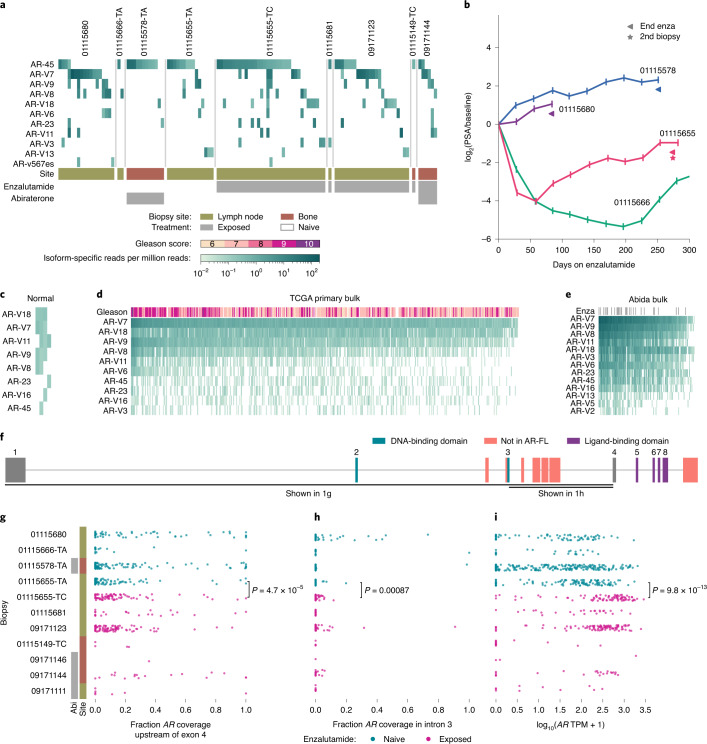
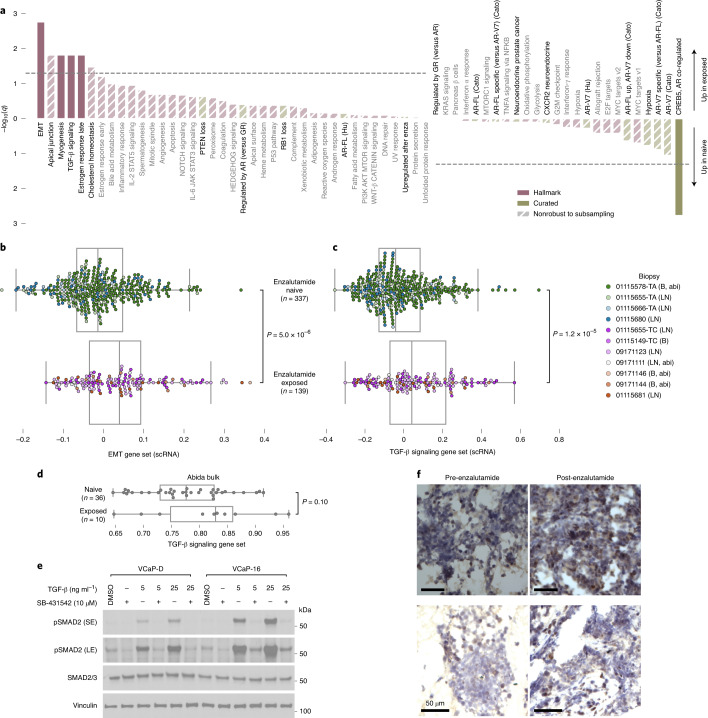
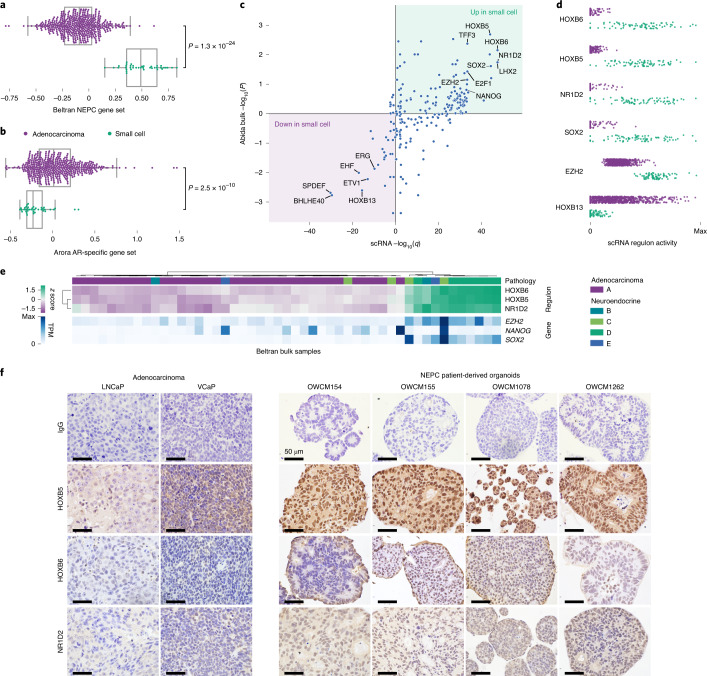
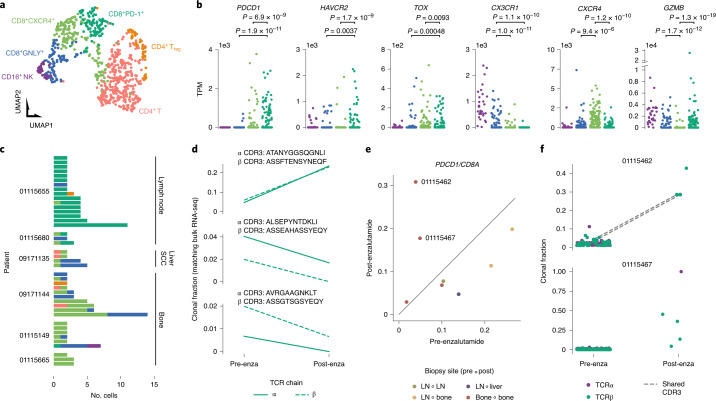
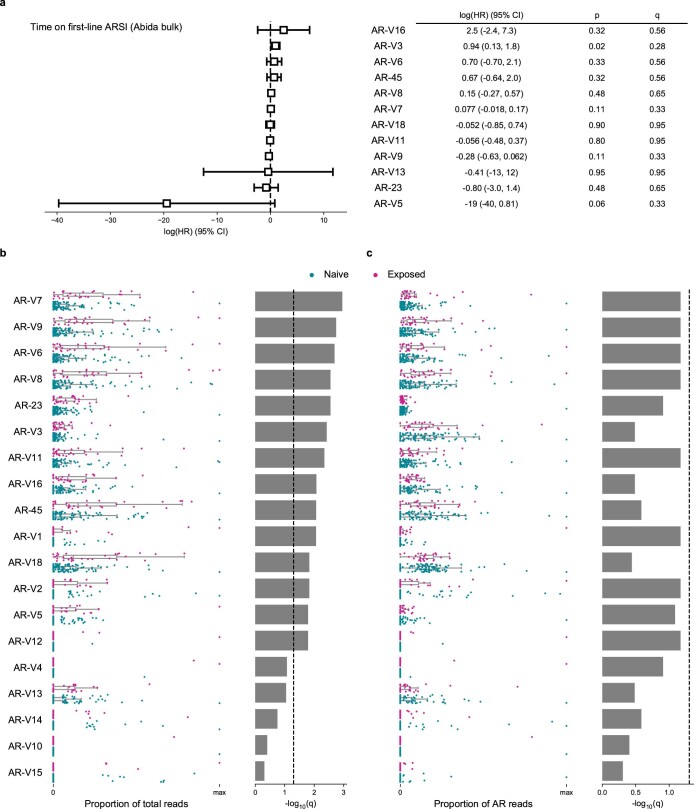
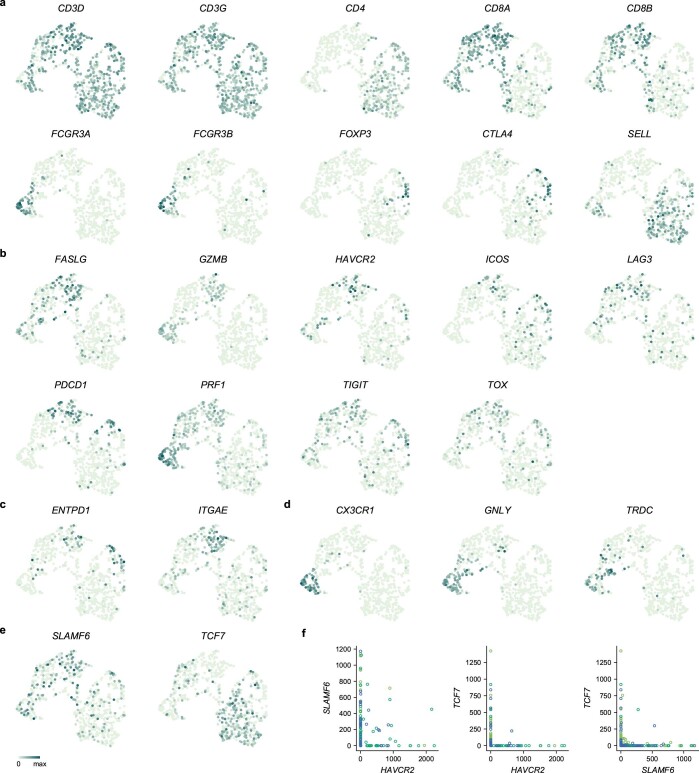
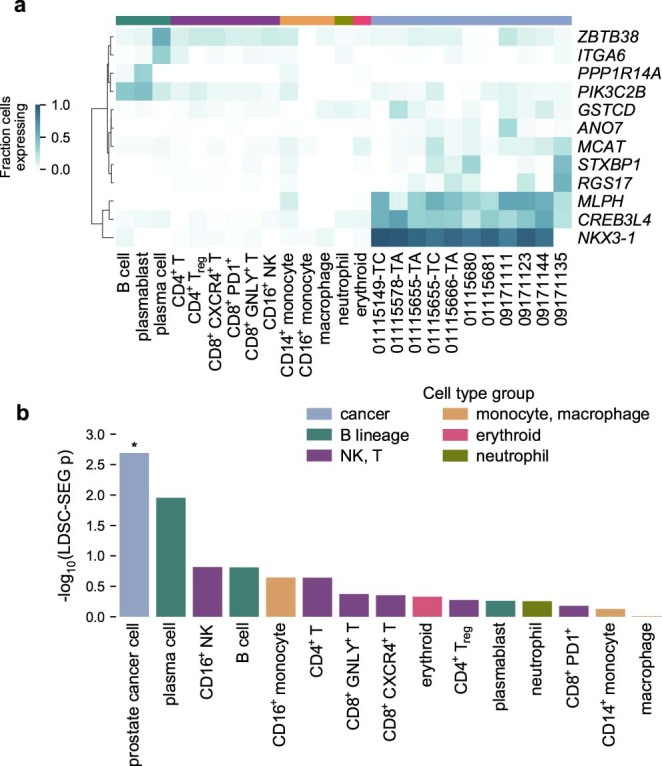
Metastatic castration-resistant prostate cancer is typically lethal, exhibiting intrinsic or acquired resistance to second-generation androgen-targeting therapies and minimal response to immune checkpoint inhibitors1. Cellular programs driving resistance in both cancer and immune cells remain poorly understood. We present single-cell transcriptomes from 14 patients with advanced prostate cancer, spanning all common metastatic sites. Irrespective of treatment exposure, adenocarcinoma cells pervasively coexpressed multiple androgen receptor isoforms, including truncated isoforms hypothesized to mediate resistance to androgen-targeting therapies2,3. Resistance to enzalutamide was associated with cancer cell-intrinsic epithelial-mesenchymal transition and transforming growth factor-β signaling. Small cell carcinoma cells exhibited divergent expression programs driven by transcriptional regulators promoting lineage plasticity and HOXB5, HOXB6 and NR1D2 (refs. 4-6). Additionally, a subset of patients had high expression of dysfunction markers on cytotoxic CD8+ T cells undergoing clonal expansion following enzalutamide treatment. Collectively, the transcriptional characterization of cancer and immune cells from human metastatic castration-resistant prostate cancer provides a basis for the development of therapeutic approaches complementing androgen signaling inhibition.
Conflict of interest statement
M.X.H. has been a consultant to Amplify Medicines and Ikena Oncology. Z.B. reports research support from Bristol-Meyers Squibb (BMS) and Genentech/imCORE unrelated to the current study. B.I. is a consultant for Merck and Volastra Therapeutics. D.L. reports funding by a postdoctoral fellowship from the Society for Immunotherapy of Cancer, which is funded in part by an educational grant from BMS. BMS has had no input into the conception, conduct or reporting of the submitted work. N.I.V. has served on an advisory board for Sanofi/Genzyme and is supported by a grant from the Society of Immunotherapy of Cancer that is funded in part by Genentech. L.F. reports receiving commercial research grants from AbbVie, Bavarian Nordic, BMS, Dendreon, Janssen, Merck and Roche/Genentech. S.P.B. served as an advisor for Sanofi. H.B. reports advisory/consulting from Janssen, Amgen, Astra Zeneca, Pfizer, Astellas, Sanofi Genzyme and research funding from Janssen, AbbVie Stemcentryx, Eli Lilly, Millenium and Astellas. A. Regev is a founder and equity holder of Celsius Therapeutics, an equity holder in Immunitas Therapeutics and, until 31 August 2020, was a SAB member of Syros Pharmaceuticals, Neogene Therapeutics, Asimov and Thermo Fisher Scientific; from 1 August 2020, A. Regev is an employee of Genentech. A. Rotem is an employee of Astra Zeneca and an equity holder in NucleAI and Celsius Therapeutics. M.-E.T. reports advisory relationships with Celgene, Janssen, GSK/Parexel, Bayer, Astra Zeneca, Riovant, AbbVie, Arcus, Astellas, Pfizer, Constellation, Summus Global, MH Life Sciences/Intellisphere, Targeted Oncology and Aptitude Health. E.M.V.A. reports advisory relationships and consulting with Tango Therapeutics, Genome Medical, Invitae, Illumina, Enara Bio, Manifold Bio and Janssen; research support from Novartis and BMS; equity in Tango Therapeutics, Genome Medical, Syapse, Manifold Bio and Enara Bio; and travel reimbursement from Roche and Genentech, outside the submitted work.
Figures


Similar articles
-
Inhibition of protein kinase C/Twist1 signaling augments anticancer effects of androgen deprivation and enzalutamide in prostate cancer.Clin Cancer Res. 2014 Feb 15;20(4):951-61. doi: 10.1158/1078-0432.CCR-13-1809. Epub 2013 Dec 18. Clin Cancer Res. 2014. PMID: 24352647
-
Exploitation of the Androgen Receptor to Overcome Taxane Resistance in Advanced Prostate Cancer.Adv Cancer Res. 2015;127:123-58. doi: 10.1016/bs.acr.2015.03.001. Epub 2015 Mar 29. Adv Cancer Res. 2015. PMID: 26093899 Review.
-
Treating Patients with Metastatic Castration Resistant Prostate Cancer: A Comprehensive Review of Available Therapies.J Urol. 2015 Dec;194(6):1537-47. doi: 10.1016/j.juro.2015.06.106. Epub 2015 Jul 18. J Urol. 2015. PMID: 26196735 Review.
-
Targeting persistent androgen receptor signaling in castration-resistant prostate cancer.Med Oncol. 2016 May;33(5):44. doi: 10.1007/s12032-016-0759-3. Epub 2016 Apr 4. Med Oncol. 2016. PMID: 27042852 Review.
-
Molecular characterization of enzalutamide-treated bone metastatic castration-resistant prostate cancer.Eur Urol. 2015 Jan;67(1):53-60. doi: 10.1016/j.eururo.2014.05.005. Epub 2014 May 29. Eur Urol. 2015. PMID: 24882673 Free PMC article. Clinical Trial.
Cited by
-
Immune Checkpoint Inhibitors in Advanced Prostate Cancer: Current Data and Future Perspectives.Cancers (Basel). 2022 Feb 28;14(5):1245. doi: 10.3390/cancers14051245. Cancers (Basel). 2022. PMID: 35267553 Free PMC article. Review.
-
Epithelial-Mesenchymal Transition Signaling and Prostate Cancer Stem Cells: Emerging Biomarkers and Opportunities for Precision Therapeutics.Genes (Basel). 2021 Nov 27;12(12):1900. doi: 10.3390/genes12121900. Genes (Basel). 2021. PMID: 34946849 Free PMC article. Review.
-
Targeting ADAR1 with a small molecule for the treatment of prostate cancer.Nat Cancer. 2025 Mar;6(3):474-492. doi: 10.1038/s43018-025-00907-4. Epub 2025 Feb 10. Nat Cancer. 2025. PMID: 39930013
-
Single cell and spatial transcriptomics highlight the interaction of club-like cells with immunosuppressive myeloid cells in prostate cancer.Nat Commun. 2024 Nov 16;15(1):9949. doi: 10.1038/s41467-024-54364-1. Nat Commun. 2024. PMID: 39550375 Free PMC article.
-
Computer-aided drug discovery strategies for novel therapeutics for prostate cancer leveraging next-generating sequencing data.Expert Opin Drug Discov. 2024 Jul;19(7):841-853. doi: 10.1080/17460441.2024.2365370. Epub 2024 Jun 11. Expert Opin Drug Discov. 2024. PMID: 38860709 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
