

High-flow therapy: physiological effects and clinical applications
- PMID: 33664838
- PMCID: PMC7910031
- DOI: 10.1183/20734735.0224-2020
High-flow therapy: physiological effects and clinical applications
Abstract
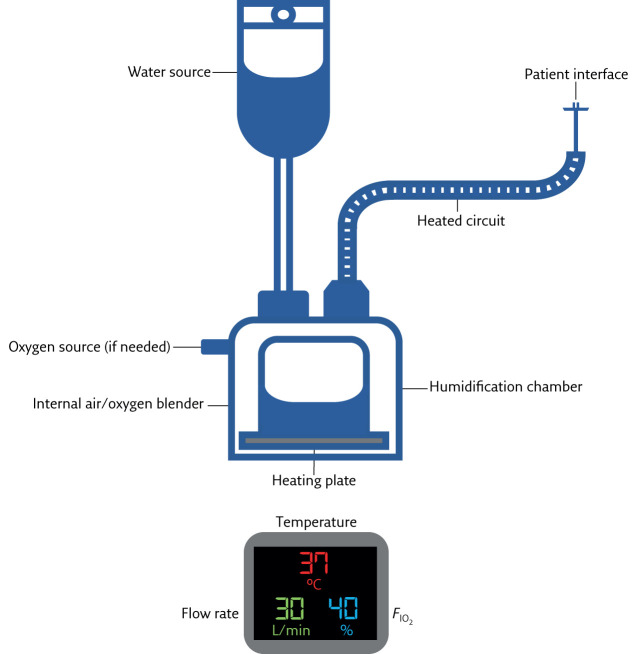
Humidified high-flow therapy (HFT) is a noninvasive respiratory therapy, typically delivered through a nasal cannula interface, which delivers a stable fraction of inspired oxygen (F IO2 ) at flow rates of up to 60 L·min-1. It is well-tolerated, simple to set up and ideally applied at 37°C to permit optimal humidification of inspired gas. Flow rate and F IO2 should be selected based on patients' inspiratory effort and severity of hypoxaemia. HFT yields beneficial physiological effects, including improved mucociliary clearance, enhanced dead space washout and optimisation of pulmonary mechanics. Robust evidence supports its application in the critical care setting (treatment of acute hypoxaemic respiratory failure and prevention of post-extubation respiratory failure) and emerging data supports HFT use during bronchoscopy, intubation and breaks from noninvasive ventilation or continuous positive airway pressure. There are limited data on HFT use in patients with hypercapnic respiratory failure, as an adjunct to pulmonary rehabilitation and in the palliative care setting, and further research is needed to validate the findings of small studies. The COVID-19 pandemic raises questions regarding HFT efficacy in COVID-19-related hypoxaemic respiratory failure and concerns regarding aerosolisation of respiratory droplets. Clinical trials are ongoing and healthcare professionals should implement strict precautions to mitigate the risk of nosocomial transmission.
Educational aims: Provide a practical guide to HFT setup and delivery.Outline the physiological effects of HFT on the respiratory system.Describe clinical applications of HFT in adult respiratory and critical care medicine and evaluate the supporting evidence.Discuss application of HFT in COVID-19 and aerosolisation of respiratory droplets.
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: R.F. D'Cruz has nothing to disclose. Conflict of interest: N. Hart reports grants from Philips-Respironics (OPIP Trial, unrestricted research grant), RESMED (HoT-HMV Trial, unrestricted research grant) and Philips-Respironics (HoT-HMV Trial, unrestricted research grant), non-financial support from Philips-Respironics RT Meeting (development of MYOTRACE technology), outside the submitted work. In addition, Prof. Hart has a European patent for MYOTRACE issued, and a US patent for MYOTRACE pending. Prof. Hart's research group has received unrestricted grants (managed by Guy's & St Thomas' Foundation Trust) from Philips and Resmed. Philips are contributing to the development of the MYOTRACE technology. Conflict of interest: G. Kaltsakas has nothing to disclose.
Figures
References
-
- Transpirator Technologies, Inc. Annual Report Form 10-KSB 2002. https://sec.report/Document/0000950144-02- 007036/
-
- Roca O, Riera J, Torres F, et al. . High-flow oxygen therapy in acute respiratory failure. Respir Care 2010; 55: 408–413. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous