

Downregulation of death receptor 4 is tightly associated with positive response of EGFR mutant lung cancer to EGFR-targeted therapy and improved prognosis
- PMID: 33664875
- PMCID: PMC7914351
- DOI: 10.7150/thno.54824
Downregulation of death receptor 4 is tightly associated with positive response of EGFR mutant lung cancer to EGFR-targeted therapy and improved prognosis
Abstract
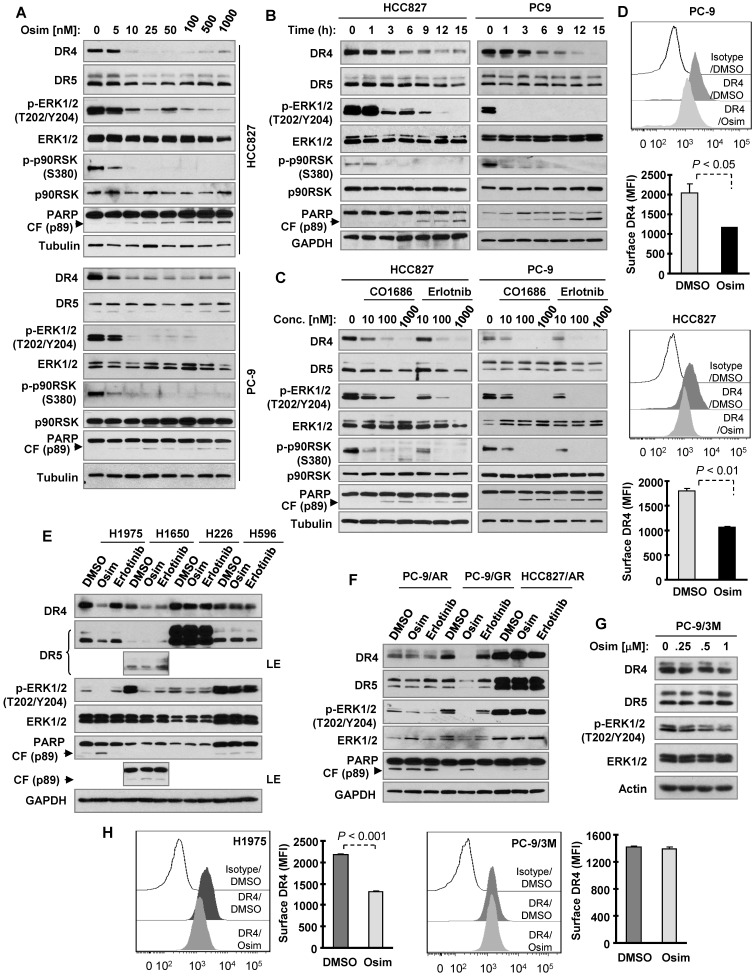
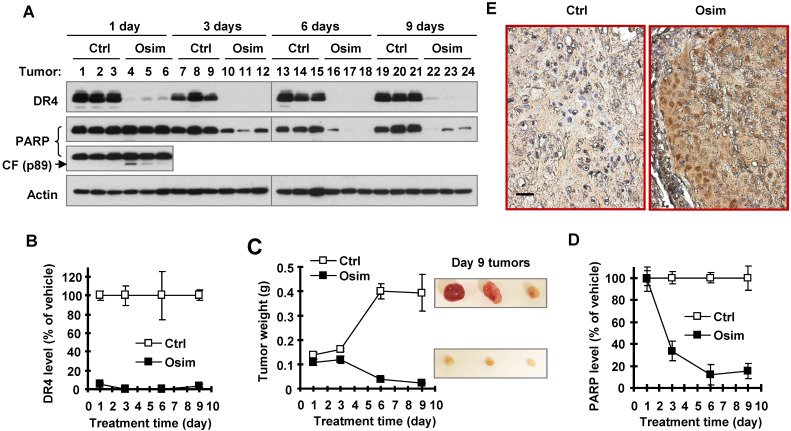
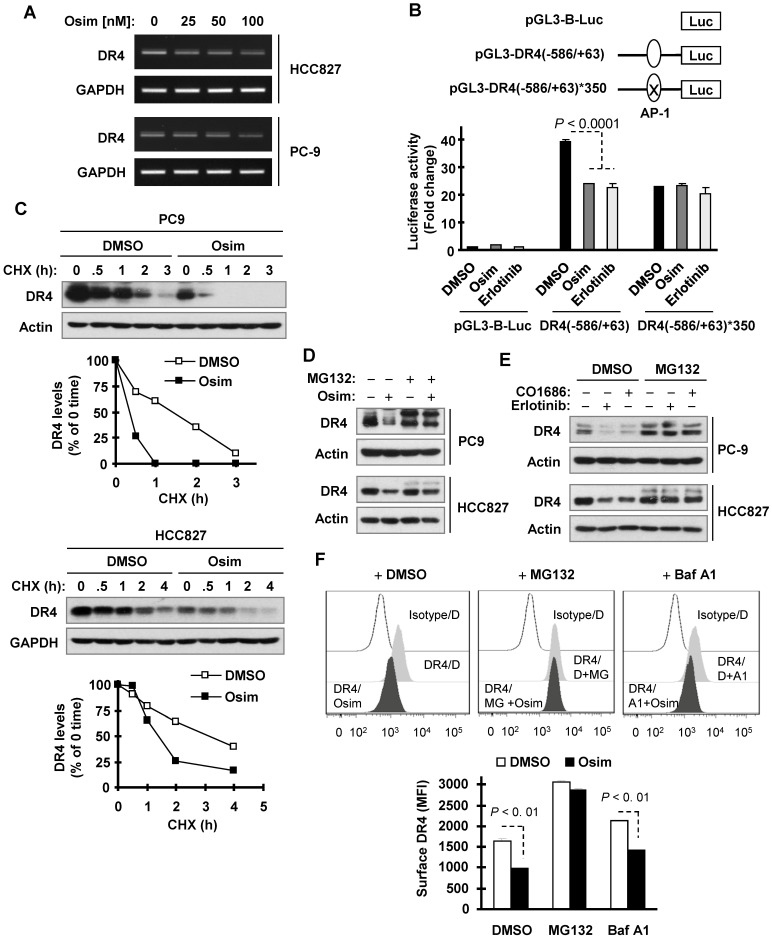
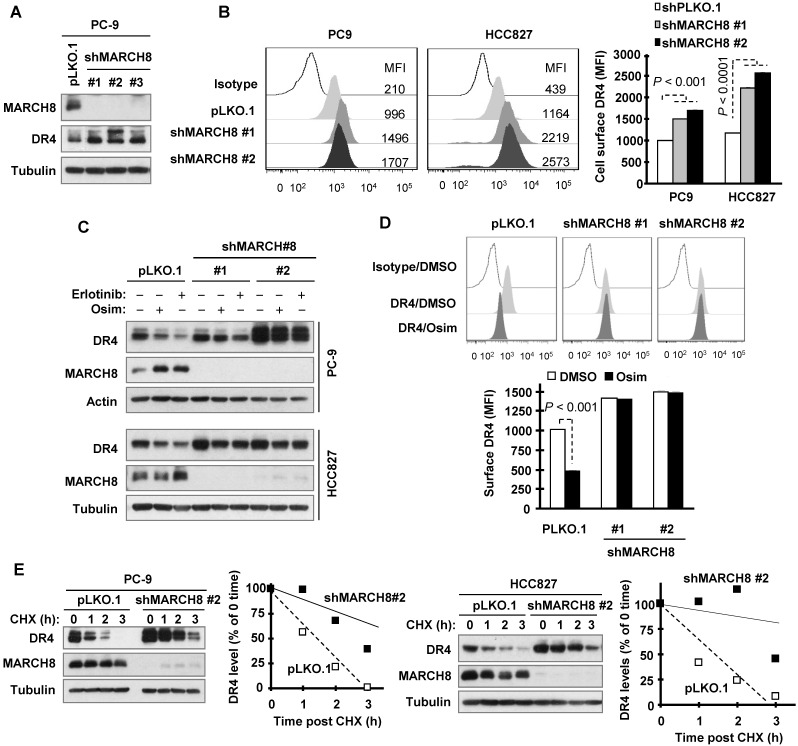
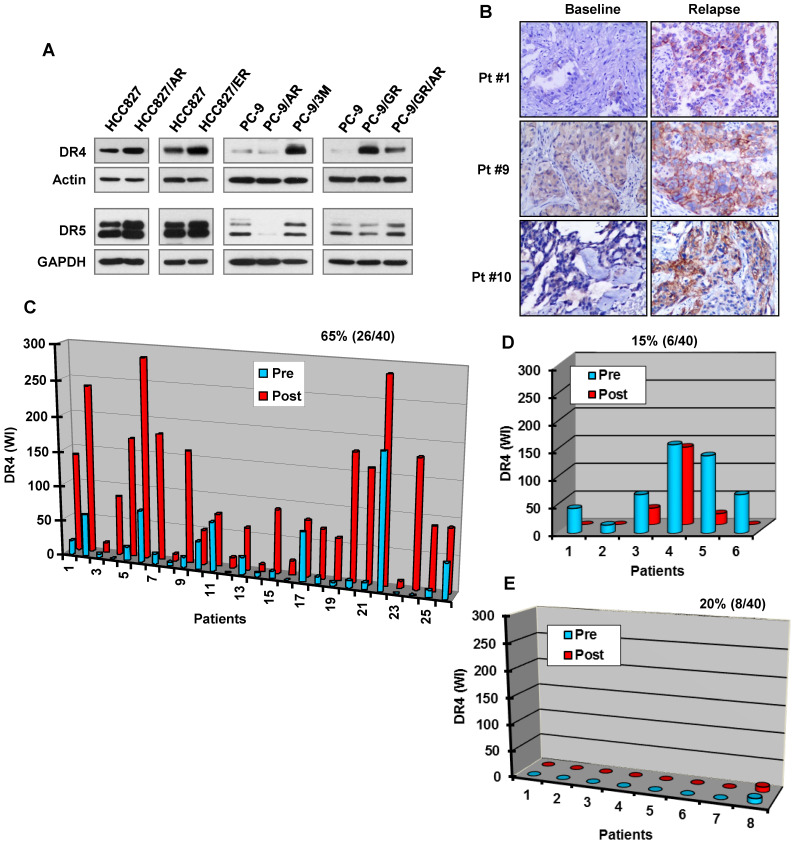
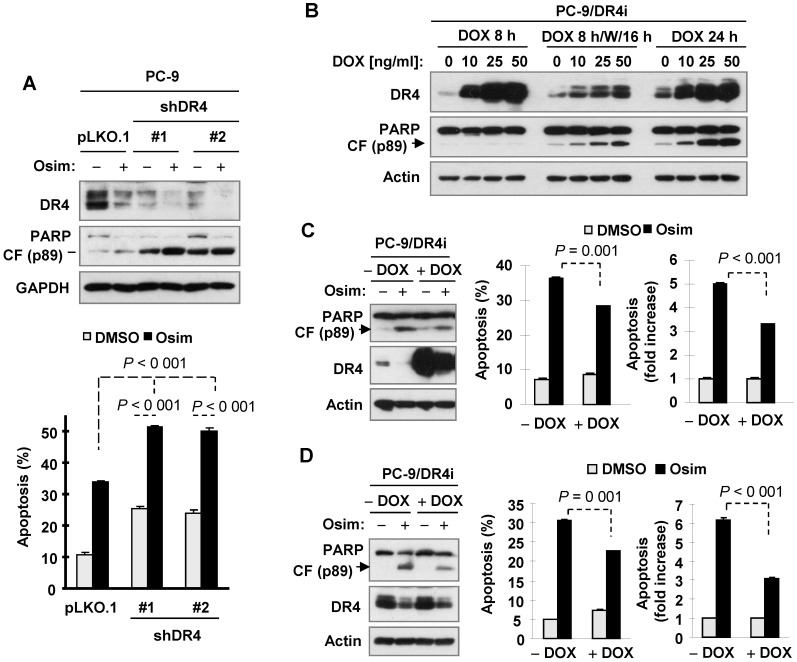
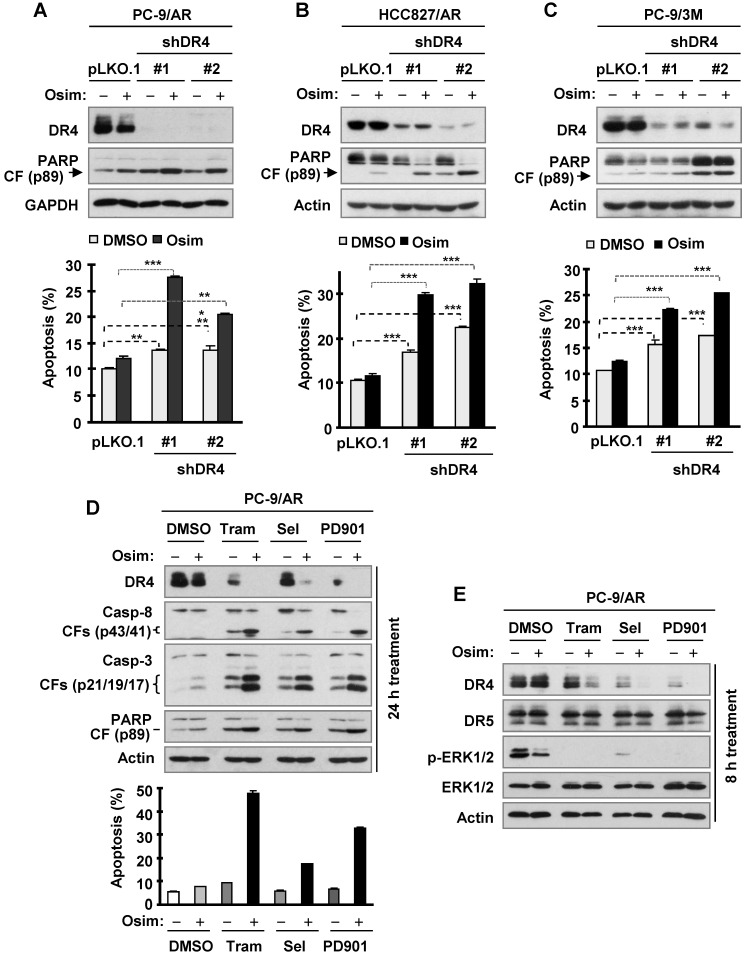
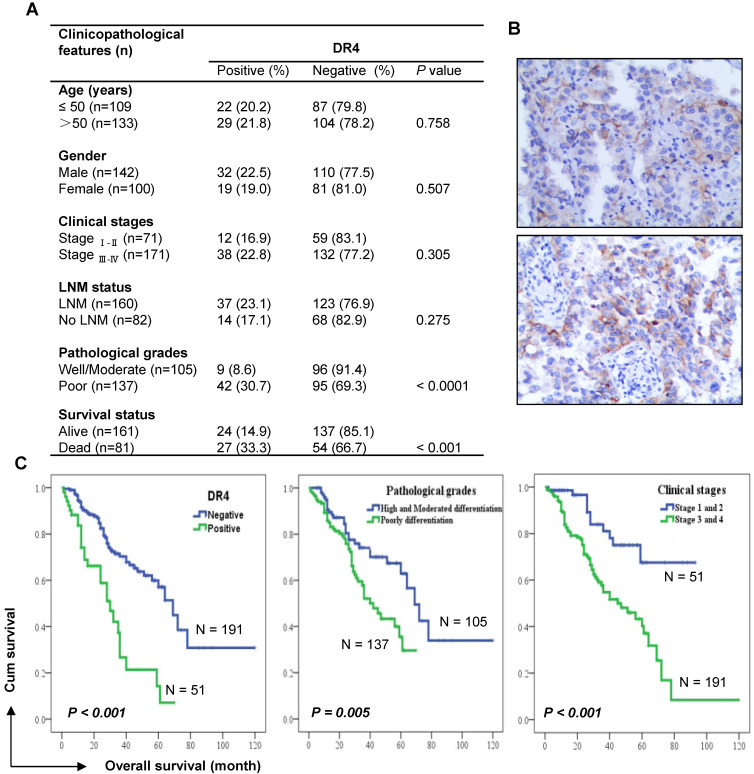
Death receptor 4 (DR4), a cell surface receptor, mediates apoptosis or induces inflammatory cytokine secretion upon binding to its ligand depending on cell contexts. Its prognostic impact in lung cancer and connection between EGFR-targeted therapy and DR4 modulation has not been reported and thus was the focus of this study. Methods: Intracellular protein alterations were measured by Western blotting. Cell surface protein was detected with antibody staining and flow cytometry. mRNA expression was monitored with qRT-PCR. Gene transactivation was analyzed with promoter reporter assay. Drug dynamic effects in vivo were evaluated using xenografts. Gene modulations were achieved with gene overexpression and knockdown. Proteins in human archived tissues were stained with immunohistochemistry. Results: EGFR inhibitors (e.g., osimertinib) decreased DR4 levels only in EGFR mutant NSCLC cells and tumors, being tightly associated with induction of apoptosis. This modulation was lost once cells became resistant to these inhibitors. Increased levels of DR4 were detected in cell lines with acquired osimertinib resistance and in NSCLC tissues relapsed from EGFR-targeted therapy. DR4 knockdown induced apoptosis and augmented apoptosis when combined with osimertinib in both sensitive and resistant cell lines, whereas enforced DR4 expression significantly attenuated osimertinib-induced apoptosis. Mechanistically, osimertinib induced MARCH8-mediated DR4 proteasomal degradation and suppressed MEK/ERK/AP-1-dependent DR4 transcription, resulting in DR4 downregulation. Moreover, we found that DR4 positive expression in human lung adenocarcinoma was significantly associated with poor patient survival. Conclusions: Collectively, we suggest that DR4 downregulation is coupled to therapeutic efficacy of EGFR-targeted therapy and predicts improved prognosis, revealing a previously undiscovered connection between EGFR-targeted therapy and DR4 modulation.
Keywords: EGFR inhibitors; acquired resistance; apoptosis; death receptor 4; osimertinib.
© The author(s).
Conflict of interest statement
Competing Interests: SSR is on consulting/advisory boards for AstraZeneca, BMS, Merck, Roche, Tesaro and Amgen. TKO is on consulting/advisory boards for Novartis, Celgene, Lilly, Sandoz, Abbvie, Eisai, Takeda, Bristol-Myers Squibb, MedImmune, Amgen, AstraZeneca and Boehringer Ingelheim. Other authors disclose no potential conflicts of interest.
Figures
Similar articles
-
Membrane-Associated RING-CH 8 Functions as a Novel PD-L1 E3 Ligase to Mediate PD-L1 Degradation Induced by EGFR Inhibitors.Mol Cancer Res. 2021 Oct;19(10):1622-1634. doi: 10.1158/1541-7786.MCR-21-0147. Epub 2021 Jun 28. Mol Cancer Res. 2021. PMID: 34183449 Free PMC article.
-
MET inhibition downregulates DR4 expression in MET-amplified lung cancer cells with acquired resistance to EGFR inhibitors through suppressing AP-1-mediated transcription.Neoplasia. 2021 Aug;23(8):766-774. doi: 10.1016/j.neo.2021.06.006. Epub 2021 Jul 4. Neoplasia. 2021. PMID: 34233230 Free PMC article.
-
Induction of IL6/STAT3-dependent TRAIL expression that contributes to the therapeutic efficacy of osimertinib in EGFR mutant NSCLC cells.Oncogene. 2025 Jul;44(27):2315-2327. doi: 10.1038/s41388-025-03381-5. Epub 2025 Apr 17. Oncogene. 2025. PMID: 40247082
-
Treatment of Brain Metastases of Non-Small Cell Lung Carcinoma.Int J Mol Sci. 2021 Jan 8;22(2):593. doi: 10.3390/ijms22020593. Int J Mol Sci. 2021. PMID: 33435596 Free PMC article. Review.
-
Osimertinib and other third-generation EGFR TKI in EGFR-mutant NSCLC patients.Ann Oncol. 2018 Jan 1;29(suppl_1):i20-i27. doi: 10.1093/annonc/mdx704. Ann Oncol. 2018. PMID: 29462255 Review.
Cited by
-
The novel BET degrader, QCA570, is highly active against the growth of human NSCLC cells and synergizes with osimertinib in suppressing osimertinib-resistant EGFR-mutant NSCLC cells.Am J Cancer Res. 2022 Feb 15;12(2):779-792. eCollection 2022. Am J Cancer Res. 2022. PMID: 35261801 Free PMC article.
-
Membrane-Associated RING-CH 8 Functions as a Novel PD-L1 E3 Ligase to Mediate PD-L1 Degradation Induced by EGFR Inhibitors.Mol Cancer Res. 2021 Oct;19(10):1622-1634. doi: 10.1158/1541-7786.MCR-21-0147. Epub 2021 Jun 28. Mol Cancer Res. 2021. PMID: 34183449 Free PMC article.
-
Optimizing Osimertinib for NSCLC: Targeting Resistance and Exploring Combination Therapeutics.Cancers (Basel). 2025 Jan 29;17(3):459. doi: 10.3390/cancers17030459. Cancers (Basel). 2025. PMID: 39941826 Free PMC article. Review.
-
Challenges of EGFR-TKIs in NSCLC and the potential role of herbs and active compounds: From mechanism to clinical practice.Front Pharmacol. 2023 Apr 7;14:1090500. doi: 10.3389/fphar.2023.1090500. eCollection 2023. Front Pharmacol. 2023. PMID: 37089959 Free PMC article. Review.
-
Targeting apoptosis to manage acquired resistance to third generation EGFR inhibitors.Front Med. 2022 Oct;16(5):701-713. doi: 10.1007/s11684-022-0951-0. Epub 2022 Sep 24. Front Med. 2022. PMID: 36152124 Review.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2018;68:394–424. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA: a cancer journal for clinicians. 2019;69:7–34. - PubMed
-
- Govindan R. Overcoming resistance to targeted therapy for lung cancer. N Engl J Med. 2015;372:1760–1. - PubMed
-
- Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH. et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378:113–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
