

Responsiveness to bepridil predicts atrial substrate in patients with persistent atrial fibrillation
- PMID: 33664889
- PMCID: PMC7896463
- DOI: 10.1002/joa3.12492
Responsiveness to bepridil predicts atrial substrate in patients with persistent atrial fibrillation
Abstract
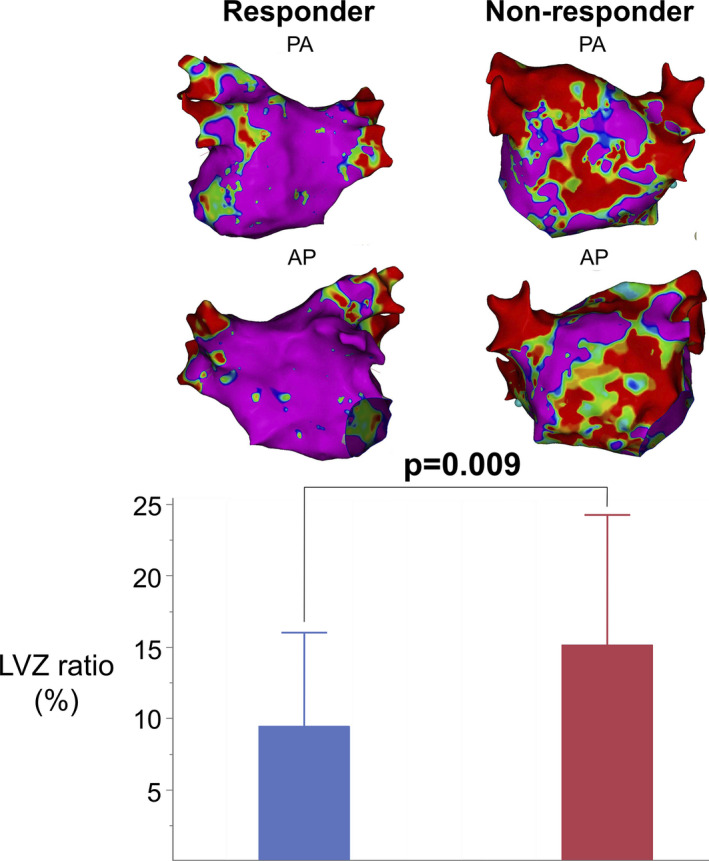
Background: The low voltage zone (LVZ) detected with three-dimensional electroanatomical mapping is a surrogate marker of atrial scar in patients with persistent atrial fibrillation (PeAF) and is associated with poor clinical outcomes after catheter ablation. However, fewer studies have reported the relationship between responsiveness to antiarrhythmic drugs and the LVZ.
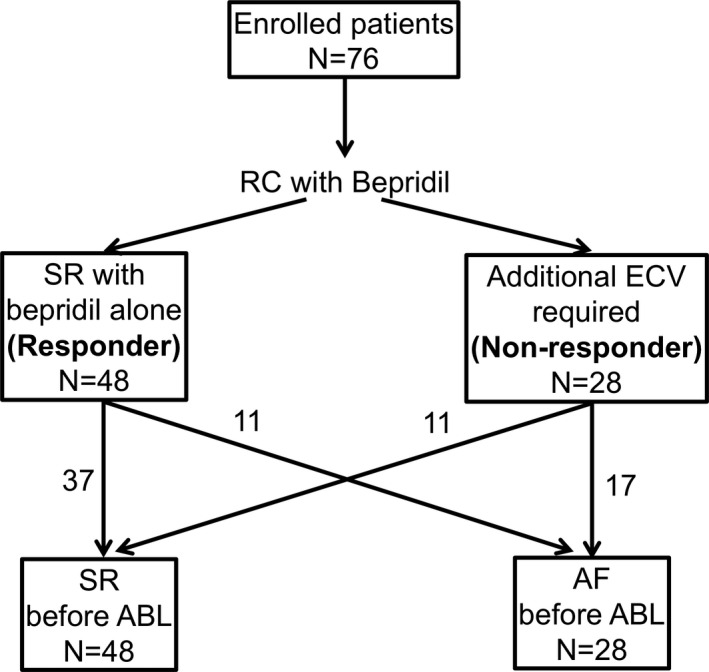
Methods: We retrospectively analyzed 76 patients who underwent catheter ablation for PeAF at our center. Rhythm control with bepridil was initiated before ablation in all patients, and electrical cardioversion was performed in cases of failure to restore sinus rhythm with bepridil alone. Patients with successful sinus restoration with bepridil alone (≤200 mg/d) were defined as "responders", while those who required electrical cardioversion as well were defined as "non-responders". We compared the LVZ ratio (ratio of the LVZ surface area to the left atrium surface area on three-dimensional electroanatomical mapping) and the recurrence-free rate after ablation between the two groups.
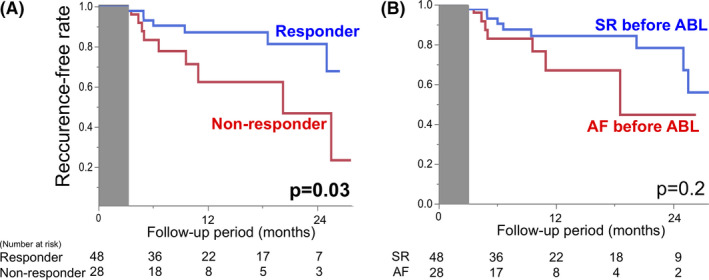
Results: Of the 76 patients, 48 (63.2%) were responders to bepridil. The median LVZ ratio was significantly lower in the responder group than in the nonresponder group (7.5% vs 14.0%, P = .009). Multivariate analysis revealed that response to bepridil was an independent predictor of normal voltage (P = .02, odds ratio = 0.20, 95% confidence interval = 0.04-0.76). The recurrence-free rate at 1 year after catheter ablation was significantly higher in the responder group than in the nonresponder group (87.1% vs 62.3%, P = .03).
Conclusions: Response to bepridil is a marker of normal voltage in electroanatomical mapping and is significantly associated with better clinical outcomes after catheter ablation.
Keywords: atrial fibrillation; atrial remodeling; bepridil hydrochloride; catheter ablation; low voltage zone.
© 2021 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Heart Rhythm Society.
Conflict of interest statement
The authors declare no conflicts of interests for this article. The protocol for this study was approved by the Ethics Committee of our center on 22 April 2020 (Approval number: 20C009).
Figures
Similar articles
-
Efficacy of hybrid therapy using prior administration of bepridil hydrochloride and cryoballoon ablation in patients with persistent atrial fibrillation.J Cardiol. 2020 Apr;75(4):360-367. doi: 10.1016/j.jjcc.2019.08.017. Epub 2019 Sep 18. J Cardiol. 2020. PMID: 31540839
-
Impact of postprocedural antiarrhythmic drug therapy with bepridil on maintaining sinus rhythm after catheter ablation for persistent atrial fibrillation.J Cardiol. 2016 Sep;68(3):229-35. doi: 10.1016/j.jjcc.2015.09.012. Epub 2015 Dec 3. J Cardiol. 2016. PMID: 26654806
-
Impact of the extent of low-voltage zone on outcomes after voltage-based catheter ablation for persistent atrial fibrillation.J Cardiol. 2018 Nov;72(5):427-433. doi: 10.1016/j.jjcc.2018.04.010. Epub 2018 May 26. J Cardiol. 2018. PMID: 29807864
-
Effect of preprocedural pharmacologic cardioversion on pulmonary vein isolation in patients with persistent atrial fibrillation.Heart Rhythm. 2021 Sep;18(9):1473-1479. doi: 10.1016/j.hrthm.2021.04.027. Epub 2021 Apr 28. Heart Rhythm. 2021. PMID: 33932587
-
Efficacy of Left Atrial Voltage-Based Catheter Ablation of Persistent Atrial Fibrillation.J Cardiovasc Electrophysiol. 2016 Sep;27(9):1055-63. doi: 10.1111/jce.13019. Epub 2016 Jun 30. J Cardiovasc Electrophysiol. 2016. PMID: 27235000
Cited by
-
Clinical insights into the role of bepridil in recurrence prevention after ablation of persistent atrial fibrillation.J Arrhythm. 2025 May 5;41(3):e70083. doi: 10.1002/joa3.70083. eCollection 2025 Jun. J Arrhythm. 2025. PMID: 40330543 Free PMC article.
-
QT Prolongation and Torsade De Pointes After Catheter Ablation for Persistent Atrial Fibrillation in a Patient With Tachycardia-Induced Cardiomyopathy: A Case Report.Cureus. 2024 Jun 4;16(6):e61640. doi: 10.7759/cureus.61640. eCollection 2024 Jun. Cureus. 2024. PMID: 38966463 Free PMC article.
References
-
- Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995;92:1954–68. - PubMed
-
- Nattel S, Burstein B, Dobrev D. Atrial remodeling and atrial fibrillation: mechanisms and implications. Circ Arrhythm Electrophysiol. 2008;1:62–73. - PubMed
-
- Nattel S, Dobrev D. The multidimensional role of calcium in atrial fibrillation pathophysiology: mechanistic insights and therapeutic opportunities. Eur Heart J. 2012;33:1870–7. - PubMed
-
- Marrouche NF, Wilber D, Hindricks G, Jais P, Akoum N, Marchlinski F, et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study. JAMA. 2014;311:498–506. - PubMed
-
- Rolf S, Kircher S, Arya A, Eitel C, Sommer P, Richter S, et al. Tailored atrial substrate modification based on low‐voltage areas in catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7:825–33. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
