

Relationship between the degree of renal dysfunction and the safety and efficacy outcomes in patients with atrial fibrillation receiving direct oral anticoagulants
- PMID: 33664890
- PMCID: PMC7896459
- DOI: 10.1002/joa3.12493
Relationship between the degree of renal dysfunction and the safety and efficacy outcomes in patients with atrial fibrillation receiving direct oral anticoagulants
Abstract
Background: The clinical evaluation of a direct oral anticoagulant (DOAC) treatment for atrial fibrillation (AF) patients with renal dysfunction has not been sufficiently studied. This study aimed to evaluate the safety and efficacy of DOACs for patients with a severely impaired renal function.
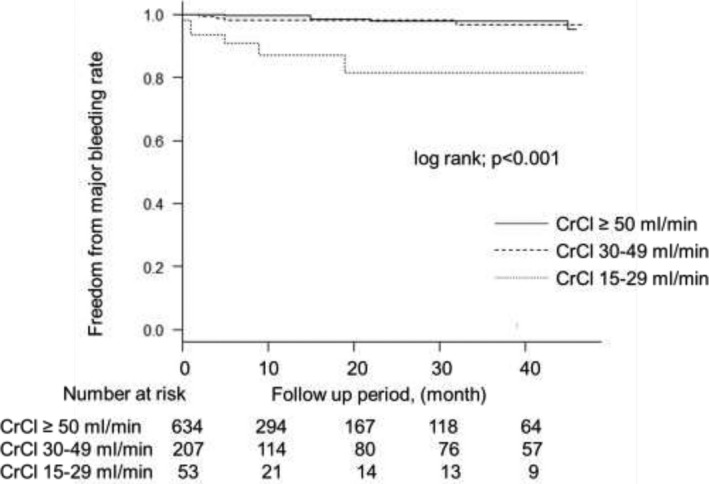
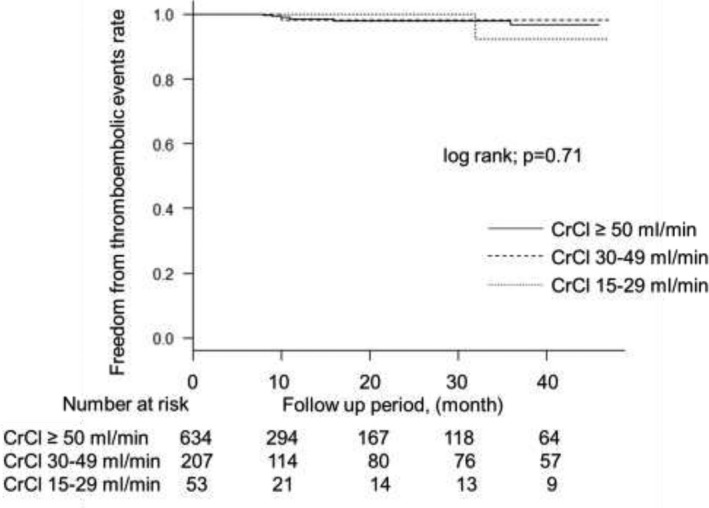
Methods: This was a retrospective and observational study in a single center. We enrolled 894 consecutive AF patients who were prescribed DOACs, and divided them into three groups based on their creatinine clearance (CrCl) value: CrCl ≥ 50 mL/min group (n = 634), CrCl 30-49 mL/min group (n = 207), and CrCl 15-29 mL/min group (n = 53). We evaluated the occurrence of major bleeding (MB) as the safety outcome and thromboembolic events (TEs) as the efficacy outcome during the follow-up.
Results: The incidence of MB in the CrCl 15-29 mL/min group was significantly higher than in the other groups (CrCl ≥ 50 mL/min group, 0.8/100 person-years; CrCl 30-49 mL/min group, 1.2/100 person-years; CrCl 15-29 mL/min group, 9.0/100 person-years, log rank test, P < .001). On the other hand, there was no significant difference in the incidence of TEs among the three groups. A multivariate analysis using a Cox proportional hazard model adjusted for the age revealed that the CrCl 15-29 mL/min group was significantly associated with increased MB compared to the CrCl ≥ 50 mL/min group (hazard ratio: 9.76, 95% confidence interval: 2.69-35.5, P < .001). Similar results were observed when adjusting for other multiple clinical factors.
Conclusion: This study demonstrated that the degree of renal dysfunction was a significant prognostic factor for MB in AF patients receiving DOACs.
Keywords: atrial fibrillation; direct oral anticoagulants; renal dysfunction.
© 2021 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Heart Rhythm Society.
Conflict of interest statement
TI has received grant support through his institution from Daiichi Sankyo and honoraria for lectures from Bayer Healthcare and Ono Pharmaceutical. Regarding this study, all authors declare that there are no potential conflicts of interest.
Figures
Similar articles
-
Renal Function and Clinical Outcomes Among Elderly Patients With Nonvalvular Atrial Fibrillation From ANAFIE.JACC Asia. 2023 Apr 11;3(3):475-487. doi: 10.1016/j.jacasi.2023.02.002. eCollection 2023 Jun. JACC Asia. 2023. PMID: 37396416 Free PMC article.
-
10-Year Trends of Antithrombotic Therapy Status and Clinical Outcomes in Patients With Atrial Fibrillation and Renal Dysfunction - The Fushimi AF Registry.Circ J. 2025 Jan 24;89(2):174-183. doi: 10.1253/circj.CJ-24-0614. Epub 2024 Oct 31. Circ J. 2025. PMID: 39477486
-
Prescription of DOACs in Patients with Atrial Fibrillation at Different Stages of Renal Insufficiency.Adv Ther. 2023 Oct;40(10):4264-4281. doi: 10.1007/s12325-023-02544-8. Epub 2023 Aug 18. Adv Ther. 2023. PMID: 37594666 Free PMC article. Review.
-
Relationship between the nutritional status and safety and efficacy outcomes in atrial fibrillation patients aged 80 years and over receiving oral anticoagulants.J Cardiol. 2021 Feb;77(2):147-153. doi: 10.1016/j.jjcc.2020.10.008. Epub 2020 Oct 22. J Cardiol. 2021. PMID: 33371946
-
Efficacy and Safety of Renal Function on Edoxaban Versus Warfarin for Atrial Fibrillation: A Systematic Review and Meta-Analysis.Medicines (Basel). 2023 Jan 16;10(1):13. doi: 10.3390/medicines10010013. Medicines (Basel). 2023. PMID: 36662497 Free PMC article. Review.
Cited by
-
Nationwide Implementation of a Population Management Dashboard for Monitoring Direct Oral Anticoagulants: Insights From the Veterans Affairs Health System.Circ Cardiovasc Qual Outcomes. 2023 Feb;16(2):e009256. doi: 10.1161/CIRCOUTCOMES.122.009256. Epub 2022 Dec 9. Circ Cardiovasc Qual Outcomes. 2023. PMID: 36484253 Free PMC article.
References
-
- Marinigh R, Lane DA, Lip GYH. Severe renal impairment and stroke prevention in atrial fibrillation: implications for thromboprophylaxis and bleeding risk. J Am Coll Cardiol. 2011;57:1339–48. - PubMed
-
- Olesen JB, Lip GYH, Kamper A‐L, Hommel K, Køber L, Lane DA, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367:625–35. - PubMed
-
- Bonde AN, Lip GYH, Kamper A‐L, Fosbøl EL, Staerk L, Carlson N, et al. Renal function and the risk of stroke and bleeding in patients with atrial fibrillation: an observational cohort study. Stroke. 2016;47:2707–13. - PubMed
-
- Bonde AN, Lip GY, Kamper AL, Hansen PR, Lamberts M, Hommel K, et al. Net clinical benefit of antithrombotic therapy in patients with atrial fibrillation and chronic kidney disease: a nationwide observational cohort study. J Am Coll Cardiol. 2014;64:2471–82. - PubMed
-
- Dahal K, Kunwar S, Rijal J, Schulman P, Lee J. Stroke, major bleeding, and mortality outcomes in warfarin users with atrial fibrillation and chronic kidney disease: a meta‐analysis of observational studies. Chest. 2016;149:951–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
