

Current status and role of programmed ventricular stimulation in patients without sustained ventricular arrhythmias and reduced ejection fraction: Analysis of the Japan cardiac device treatment registry database
- PMID: 33664897
- PMCID: PMC7896472
- DOI: 10.1002/joa3.12468
Current status and role of programmed ventricular stimulation in patients without sustained ventricular arrhythmias and reduced ejection fraction: Analysis of the Japan cardiac device treatment registry database
Abstract
Background: The aim of this study was to clarify the current status and role of programmed ventricular stimulation in patients without sustained ventricular arrhythmias and reduced left ventricular ejection fraction (LVEF).
Methods: The follow-up data of the Japan cardiac device treatment registry (JCDTR) was analyzed in 746 patients with LVEF ≦35% and no prior history of sustained ventricular arrhythmias who underwent de novo implantable cardioverter-defibrillator (ICD) or cardiac resynchronization therapy with a defibrillator (CRT-D) implantation between January 2011 and August 2015.
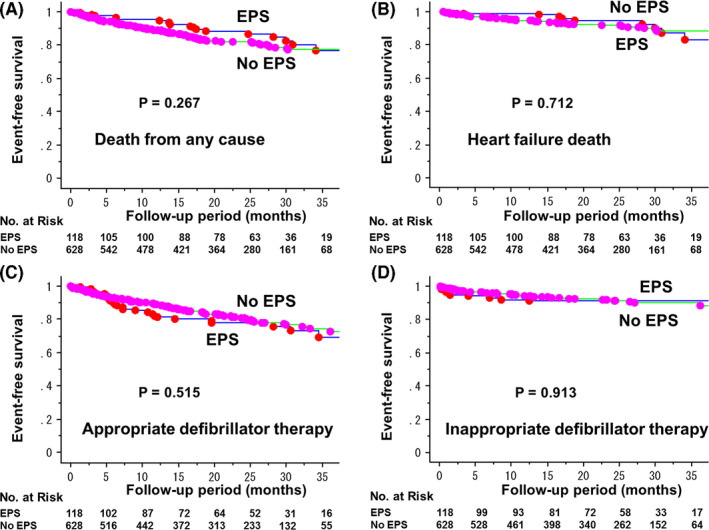
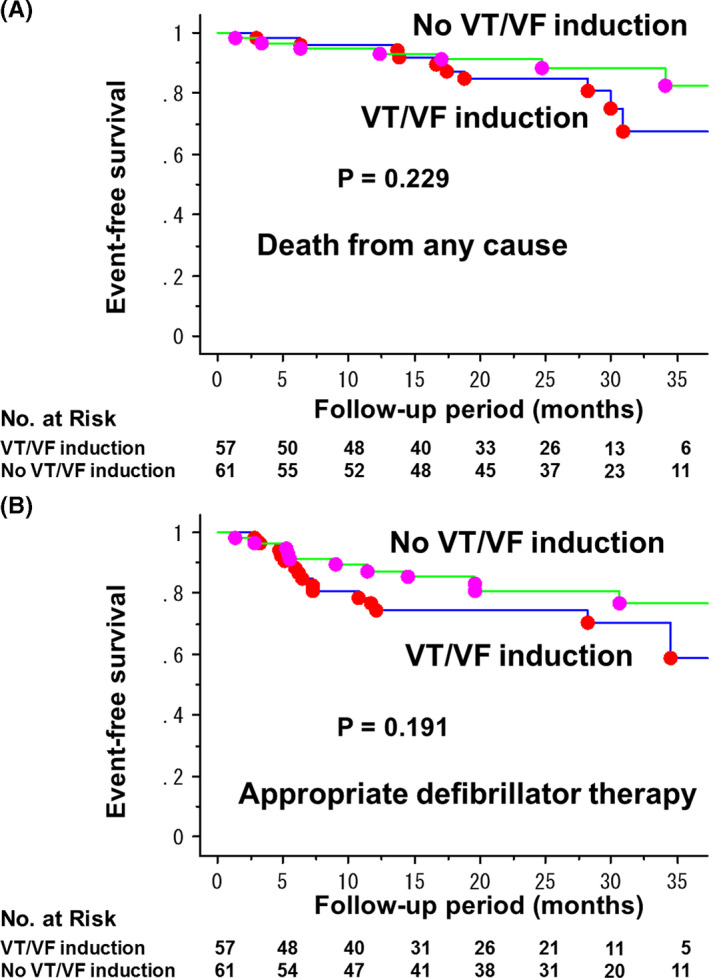
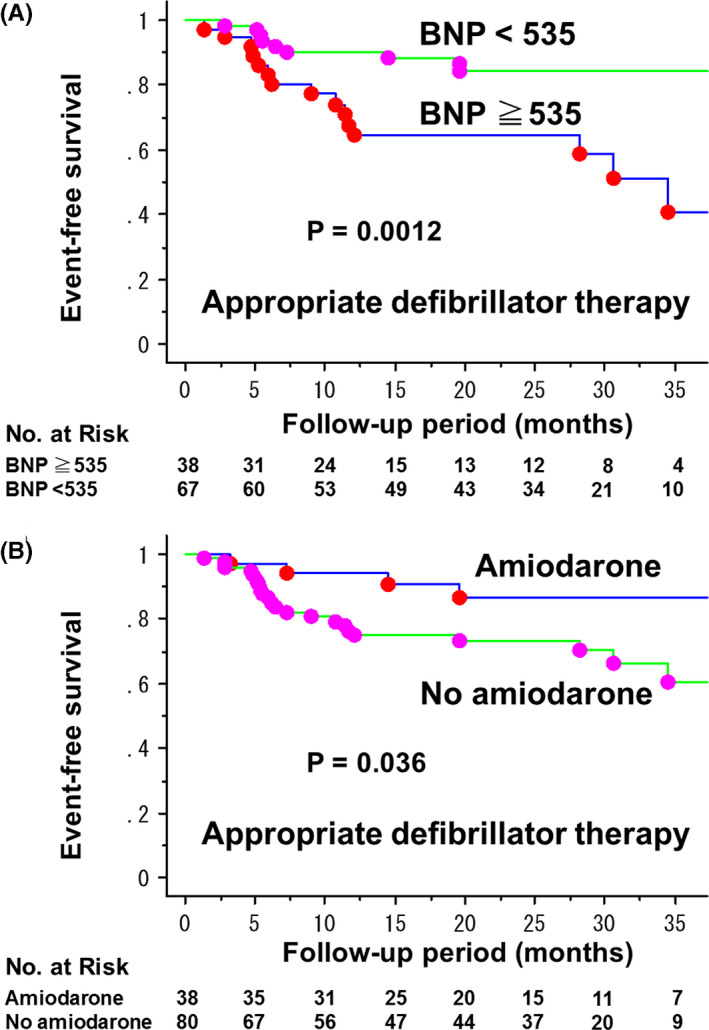
Results: Electrophysiological study (EPS) with programmed ventricular stimulation had been performed before the device implant in 118 patients (15.8%, EPS group). During the mean follow-up of 21 ± 12 months, the rate of freedom from any death and appropriate defibrillator therapy was not significantly different between EPS group (n = 118) and No EPS group (n = 628). NYHA class II-IV, and QRS duration were negatively associated with performing EPS. Among patients in the EPS group, the rate of ventricular tachycardia (VT)/ventricular fibrillation (VF) induction was 48%. The inducibility was not a predictor of appropriate defibrillator therapy, whereas BNP ≧535 pg/mL and no use of amiodarone were significantly associated with a risk of the appropriate therapy.
Conclusion: EPS for induction of VT/VF had been performed in about 16% of patients with reduced LVEF before primary prevention ICD/CRT-D implantation. Elevated BNP levels and no use of amiodarone, but not inducibility of VT/VF, appeared to be associated with appropriate defibrillator therapy in these populations.
Keywords: cardiac resynchronization therapy with a defibrillator (CRT‐D); electrophysiological study (EPS); implantable cardioverter‐defibrillator (ICD); primary prevention; ventricular fibrillation (VF); ventricular tachycardia (VT).
© 2020 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Heart Rhythm Society.
Conflict of interest statement
All authors declare no conflict of interest related to this study.
Figures
Similar articles
-
Ventricular tachyarrhythmia recurrence in primary versus secondary implantable cardioverter-defibrillator patients and role of electrophysiology study.J Interv Card Electrophysiol. 2014 Dec;41(3):195-202. doi: 10.1007/s10840-014-9941-8. Epub 2014 Sep 30. J Interv Card Electrophysiol. 2014. PMID: 25267274 Clinical Trial.
-
Appropriate implantable cardioverter-defibrillator interventions in cardiac resynchronization therapy-defibrillator (CRT-D) patients undergoing device replacement: time to downgrade from CRT-D to CRT-pacemaker? Insights from real-world clinical practice in the DECODE CRT-D analysis.Europace. 2018 Sep 1;20(9):1475-1483. doi: 10.1093/europace/eux323. Europace. 2018. PMID: 29186401
-
Impact of the right ventricular lead position on clinical outcome and on the incidence of ventricular tachyarrhythmias in patients with CRT-D.Heart Rhythm. 2013 Dec;10(12):1770-7. doi: 10.1016/j.hrthm.2013.08.020. Epub 2013 Aug 22. Heart Rhythm. 2013. PMID: 23973954 Clinical Trial.
-
Response of right ventricular size to treatment with cardiac resynchronization therapy and the risk of ventricular tachyarrhythmias in MADIT-CRT.Heart Rhythm. 2013 Oct;10(10):1471-7. doi: 10.1016/j.hrthm.2013.07.029. Epub 2013 Jul 19. Heart Rhythm. 2013. PMID: 23872690 Clinical Trial.
-
Primary prevention implantable cardioverter defibrillator in cardiac resynchronization therapy recipients with advanced chronic kidney disease.Front Cardiovasc Med. 2023 Aug 23;10:1237118. doi: 10.3389/fcvm.2023.1237118. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37680559 Free PMC article.
Cited by
-
Survival benefit of primary prevention implantable cardioverter-defibrillator/cardiac resynchronization therapy with a defibrillator: Analysis of the Japan cardiac device treatment registry and Japanese cardiac registry of heart failure in cardiology.J Arrhythm. 2025 May 12;41(3):e70084. doi: 10.1002/joa3.70084. eCollection 2025 Jun. J Arrhythm. 2025. PMID: 40357355 Free PMC article.
-
Cardiac resynchronization therapy with a defibrillator in non-ischemic and ischemic patients for primary and secondary prevention of sudden cardiac death: Analysis of the Japan cardiac device treatment registry database.J Arrhythm. 2023 Aug 24;39(5):757-765. doi: 10.1002/joa3.12916. eCollection 2023 Oct. J Arrhythm. 2023. PMID: 37799798 Free PMC article.
References
-
- Buxton AE, Lee KL, DiCarlo L, Gold MR, Greer GS, Prystowsky EN, et al. Electrophysiologic testing to identify patients with coronary artery disease who are at risk for sudden death. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 2000;342(26):1937–45. - PubMed
-
- Buxton AE, Lee KL, Hafley GE, Wyse DG, Fisher JD, Lehmann MH, et al. Relation of ejection fraction and inducible ventricular tachycardia to mode of death in patients with coronary artery disease: an analysis of patients enrolled in the Multicenter Unsustained Tachycardia Trial. Circulation. 2002;106(19):2466–72. - PubMed
-
- Grimm W, Hoffmann J, Menz V, Luck K, Maisch B. Programmed ventricular stimulation for arrhythmia risk prediction in patients with idiopathic dilated cardiomyopathy and nonsustained ventricular tachycardia. J Am Coll Cardiol. 1998;32(3):739–45. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverter‐defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225–37. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346(12):877–83. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
