

Energy loss by right ventricular pacing: Patients with versus without hypertrophic cardiomyopathy
- PMID: 33664904
- PMCID: PMC7896474
- DOI: 10.1002/joa3.12472
Energy loss by right ventricular pacing: Patients with versus without hypertrophic cardiomyopathy
Abstract
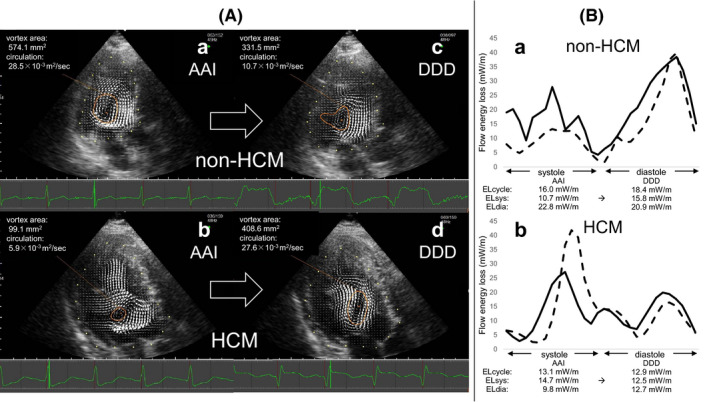
Background: Right ventricular (RV) pacing causes left ventricular (LV) dyssynchrony sometimes resulting in pacing-induced cardiomyopathy. However, RV pacing for hypertrophic obstructive cardiomyopathy is one of the treatment options. LV flow energy loss (EL) using vector flow mapping (VFM) is a novel hemodynamic index for assessing cardiac function. Our study aimed to elucidate the impact of RV pacing on EL in normal LV function and hypertrophic cardiomyopathy (HCM) patients.
Methods: A total of 36 patients with dual-chamber pacemakers for sick sinus syndrome or implantable cardioverter defibrillators for fatal ventricular tachyarrhythmias were enrolled. All patients were divided into two groups: 16 patients with HCM (HCM group) and others (non-HCM group). The absolute changes in EL under AAI (without RV pacing) and DDD (with RV pacing) modes were assessed using VFM on color Doppler echocardiography.
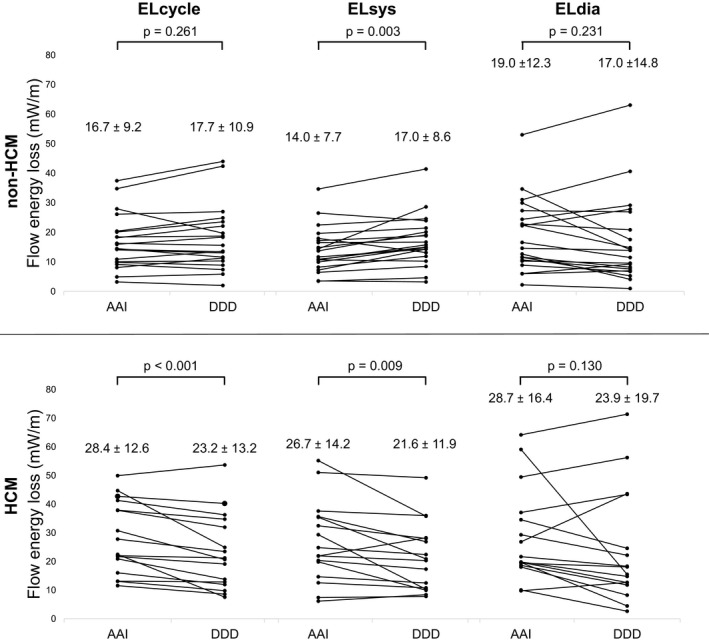
Results: In the non-HCM group, the mean systolic EL significantly increased from the AAI to DDD modes (14.0 ± 7.7 to 17.0 ± 8.6 mW/m, P = .003), whereas the mean diastolic EL did not change (19.0 ± 12.3 to 17.0 ± 14.8 mW/m, P = .231). In the HCM group, the mean systolic EL significantly decreased from the AAI to DDD modes (26.7 ± 14.2 to 21.6 ± 11.9 mW/m, P < .001), whereas the mean diastolic EL did not change (28.7 ± 16.4 to 23.9 ± 19.7 mW/m, P = .130).
Conclusions: RV pacing increased the mean systolic EL in patients without HCM. Conversely, RV pacing decreased the mean systolic EL in patients with HCM.
Keywords: echocardiography; energy loss; hypertrophic cardiomyopathy; right ventricular pacing; vector flow mapping.
© 2020 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Heart Rhythm Society.
Conflict of interest statement
The authors declares that there are no conflicts of interest related to this study.
Figures

Similar articles
-
Left ventricular energy loss and wall shear stress assessed by vector flow mapping in patients with hypertrophic cardiomyopathy.Int J Cardiovasc Imaging. 2018 Sep;34(9):1383-1391. doi: 10.1007/s10554-018-1348-7. Epub 2018 Apr 6. Int J Cardiovasc Imaging. 2018. PMID: 29626283
-
Long-term results of dual-chamber (DDD) pacing in obstructive hypertrophic cardiomyopathy. Evidence for progressive symptomatic and hemodynamic improvement and reduction of left ventricular hypertrophy.Circulation. 1994 Dec;90(6):2731-42. doi: 10.1161/01.cir.90.6.2731. Circulation. 1994. PMID: 7994815
-
Characterization of left ventricular cavity flow, wall stress and energy loss by color doppler vector flow mapping in children and adolescents with cardiomyopathy.Int J Cardiol Heart Vasc. 2020 Dec 25;32:100703. doi: 10.1016/j.ijcha.2020.100703. eCollection 2021 Feb. Int J Cardiol Heart Vasc. 2020. PMID: 33392387 Free PMC article.
-
Right ventricular involvement in hypertrophic cardiomyopathy: evidence and implications from current literature.Scand Cardiovasc J. 2021 Aug;55(4):195-204. doi: 10.1080/14017431.2021.1901979. Epub 2021 Mar 24. Scand Cardiovasc J. 2021. PMID: 33759664
-
Pacing in obstructive hypertrophic cardiomyopathy: a therapeutic option?Anadolu Kardiyol Derg. 2006 Dec;6 Suppl 2:49-54. Anadolu Kardiyol Derg. 2006. PMID: 17162271 Review.
References
-
- Tops LF, Schalij MJ, Bax JJ. The effects of right ventricular apical pacing on ventricular function and dyssynchrony. Implications for therapy. J Am Coll Cardiol. 2009;54:764–76. - PubMed
-
- Brignole M, Auricchio A, Baron‐Esquivias G, Bordachar P, Boriani G, Bordachar P, et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: The task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Europace. 2013;15:1070–118. - PubMed
-
- Dreger H, Maethner K, Bondke H, Baumann G, Melzer C. Pacing‐induced cardiomyopathy in patients with right ventricular stimulation for >15 years. Europace. 2012;14:238–42. - PubMed
-
- Kiehl EL, Makki T, Kumar R, Gumber D, Kwon DH, Rickard JW, et al. Incidence and predictors of right ventricular pacing‐induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm. 2016;13:2272–8. - PubMed
-
- O’Keefe JH, Abuissa H, Jones PG, Thompson RC, Bateman TM, McGhie AI, et al. Effect of chronic right ventricular apical pacing on left ventricular function. Am J Cardiol. 2005;95:771–3. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
