

Performance of an active fixation bipolar left ventricular lead vs passive fixation quadripolar leads in cardiac resynchronization therapy, a randomized trial
- PMID: 33664905
- PMCID: PMC7896457
- DOI: 10.1002/joa3.12450
Performance of an active fixation bipolar left ventricular lead vs passive fixation quadripolar leads in cardiac resynchronization therapy, a randomized trial
Abstract
Background: Usage of active fixation bipolar left ventricular (LV) leads represents an alternative approach to the more commonly used passive fixation quadripolar leads in cardiac resynchronization therapy (CRT). We compared a bipolar LV lead with a side screw for active fixation and passive fixation quadripolar LV leads.
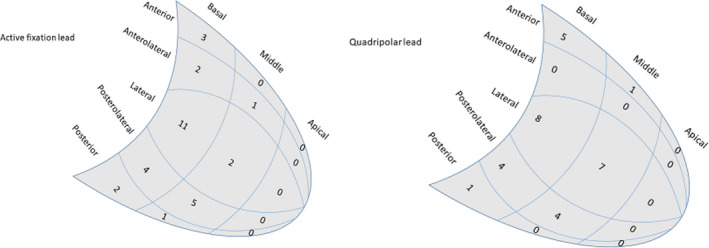
Methods: Sixty-two patients were before CRT implantations randomly allocated to receive a bipolar (n = 31) or quadripolar (n = 31) LV leads. Speckle-tracking radial strain echocardiography was used to define the LV segment with latest mechanical activation as the target LV segment. The electrophysiological measurements and the capability to obtain a proximal position in a coronary vein placed over the target segment were assessed.
Results: Upon implantation, the quadripolar lead demonstrated a lower pacing capture threshold than the bipolar lead, but at follow-up, there was no difference. There were no differences in the LV lead implant times or radiation doses. The success rate in reaching the target location was not significantly different between the two LV leads.
Conclusions: The pacing capture thresholds were low, with no significant difference between active fixation bipolar leads and quadripolar leads. Active fixation leads did not promote a more proximal location of the stimulating electrode or a higher grade of concordance to the target segment than passive fixation leads.
Keywords: biventricular pacemaker; cardiac resynchronization therapy; heart failure.
© 2020 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of Japanese Heart Rhythm Society.
Conflict of interest statement
The authors have no conflict of interest, financial or otherwise.
Figures
Similar articles
-
Clinical outcome of cardiac resynchronization therapy in patients randomized to an active fixation bipolar left ventricular lead versus a passive quadripolar lead.Scand Cardiovasc J. 2021 Jun;55(3):153-159. doi: 10.1080/14017431.2020.1869299. Epub 2021 Jan 10. Scand Cardiovasc J. 2021. PMID: 33426938 Clinical Trial.
-
Improved implant and postoperative lead performance in CRT-D patients implanted with a quadripolar left ventricular lead. A 6-month follow-up analysis from a multicenter prospective comparative study.J Interv Card Electrophysiol. 2015 Jan;42(1):59-66. doi: 10.1007/s10840-014-9956-1. Epub 2014 Dec 13. J Interv Card Electrophysiol. 2015. PMID: 25504267 Clinical Trial.
-
Long-term follow-up of patients with a quadripolar active fixation left ventricular lead: An Italian multicenter experience.J Cardiovasc Electrophysiol. 2022 Jul;33(7):1567-1575. doi: 10.1111/jce.15574. Epub 2022 Jun 11. J Cardiovasc Electrophysiol. 2022. PMID: 35634866
-
Quadripolar Leads in Cardiac Resynchronization Therapy.JACC Clin Electrophysiol. 2015 Aug;1(4):225-237. doi: 10.1016/j.jacep.2015.07.004. Epub 2015 Jul 17. JACC Clin Electrophysiol. 2015. PMID: 29759311 Review.
-
Bipolar versus quadripolar left ventricular leads for cardiac resynchronization therapy: evidence to date.Expert Rev Cardiovasc Ther. 2021 Dec;19(12):1075-1084. doi: 10.1080/14779072.2021.2013813. Expert Rev Cardiovasc Ther. 2021. PMID: 34865590 Review.
Cited by
-
Novel lead anchor technique using an active fixation quadripolar left ventricular lead in cardiac resynchronization therapy.Clin Case Rep. 2022 Feb 2;10(2):e05332. doi: 10.1002/ccr3.5332. eCollection 2022 Feb. Clin Case Rep. 2022. PMID: 35140949 Free PMC article.
-
Efficacy and safety of novel left ventricular pacing leads: 1-year analysis of the NAVIGATOR trial.Open Heart. 2024 Feb 5;11(1):e002517. doi: 10.1136/openhrt-2023-002517. Open Heart. 2024. PMID: 38316493 Free PMC article.
References
-
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002;346(24):1845–53. - PubMed
-
- Cleland JGF, Daubert J‐C, Erdmann E, Freemantle N, Gras D, Kappenberger L, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352(15):1539–49. - PubMed
-
- Goldenberg I, Moss AJ, Hall WJ, Foster E, Goldberger JJ, Santucci P, et al. Predictors of response to cardiac resynchronization therapy in the Multicenter Automatic Defibrillator Implantation Trial with Cardiac Resynchronization Therapy (MADIT‐CRT). Circulation. 2011;124(14):1527–36. - PubMed
-
- Singh JP, Klein HU, Huang DT, Reek S, Kuniss M, Quesada A, et al. Left ventricular lead position and clinical outcome in the multicenter automatic defibrillator implantation trial‐cardiac resynchronization therapy (MADIT‐CRT) trial. Circulation. 2011;123(11):1159–66. - PubMed
-
- Ypenburg C, van Bommel RJ, Delgado V, Mollema SA, Bleeker GB, Boersma E, et al. Optimal left ventricular lead position predicts reverse remodeling and survival after cardiac resynchronization therapy. J Am Coll Cardiol. 2008;52(17):1402–9. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
