

Atrial fibrillation and the risk of 30-day incident thromboembolic events, and mortality in adults ≥ 50 years with COVID-19
- PMID: 33664908
- PMCID: PMC7896479
- DOI: 10.1002/joa3.12458
Atrial fibrillation and the risk of 30-day incident thromboembolic events, and mortality in adults ≥ 50 years with COVID-19
Abstract
Background: There are limited data on the outcomes of adults with coronavirus disease 2019 (COVID-19) and atrial fibrillation (AF). The objectives were to (i) examine associations between AF, 30-day thromboembolic events and mortality in adults with COVID-19 and (ii) examine associations between COVID-19, 30-day thromboembolic events and mortality in adults with AF.
Methods: A study was conducted using a global federated health research network. Adults aged ≥50 years who presented to 41 participating healthcare organizations between 20 January 2020 and 1 September 2020 with COVID-19 were included.
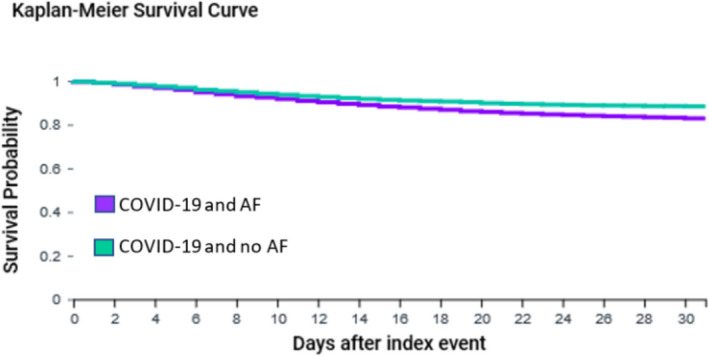
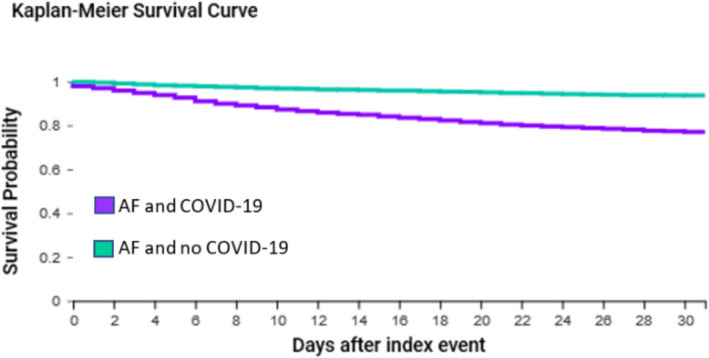
Results: For the first objective, 6589 adults with COVID-19 and AF were propensity score matched for age, gender, race, and comorbidities to 6589 adults with COVID-19 without AF. The survival probability was significantly lower in adults with COVID-19 and AF compared to matched adults without AF (82.7% compared to 88.3%, Log-Rank test P < .0001; Risk Ratio (95% confidence interval) 1.61 (1.46, 1.78)) and risk of thromboembolic events was higher in patients with AF (9.9% vs 7.0%, Log-Rank test P < .0001; Risk Ratio (95% confidence interval) 1.41 (1.26, 1.59)). For the second objective, 2454 adults with AF and COVID-19 were propensity score matched to 2454 adults with AF without COVID-19. The survival probability was significantly lower for adults with AF and COVID-19 compared to adults with AF without COVID-19, but there was no significant difference in risk of thromboembolic events.
Conclusions: AF could be an important risk factor for short-term mortality with COVID-19, and COVID-19 may increase risk of short-term mortality amongst adults with AF.
Keywords: COVID‐19; atrial fibrillation; coronavirus‐2019; mortality; thromboembolic events.
© 2020 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Heart Rhythm Society.
Conflict of interest statement
Stephanie L Harrison: None declared. Elnara Fazio‐Eynullayeva and Paula Underhill are employees of TriNetX Inc Deirdre A Lane has received investigator‐initiated educational grants from Bristol‐Myers Squibb (BMS), has been a speaker for Boehringer Ingeheim and BMS/Pfizer, and has consulted for BMS, Boehringer Ingelheim, and Daiichi‐Sankyo. Gregory Lip: consultant for Bayer/Janssen, BMS/Pfizer, Medtronic, Boehringer Ingelheim, Novartis, Verseon, and Daiichi‐Sankyo and speaker for Bayer, BMS/Pfizer, Medtronic, Boehringer Ingelheim, and Daiichi‐Sankyo. No fees are directly received to Gregory Lip personally.
Figures
References
-
- World Health Organization . Novel Coronavirus (2019‐nCoV) Situation Report ‐ 11. 2020. [cited 07/07/2020]. Available from https://www.who.int/docs/default‐source/coronaviruse/situation‐reports/2...
-
- European Centre for Disease Prevention and Control . Situation update worldwide, as of 5 August 2020. [cited 04/05/2020]. Available from https://www.ecdc.europa.eu/en/geographical‐distribution‐2019‐ncov‐cases
LinkOut - more resources
Full Text Sources
