

The role of angioembolization and C-clamp fixation: Damaged control orthopaedic in haemodynamically unstable pelvic fracture
- PMID: 33664945
- PMCID: PMC7903064
- DOI: 10.1016/j.amsu.2021.02.003
The role of angioembolization and C-clamp fixation: Damaged control orthopaedic in haemodynamically unstable pelvic fracture
Abstract
Introduction: Unstable pelvic fracture may emerge to major bleeding complication. Angioembolization is one of method to stop the bleeding effectively. This case series aims to analyze whether the bleeding of unstable pelvic fracture is managed by angioembolization to achieve the better functional outcome.
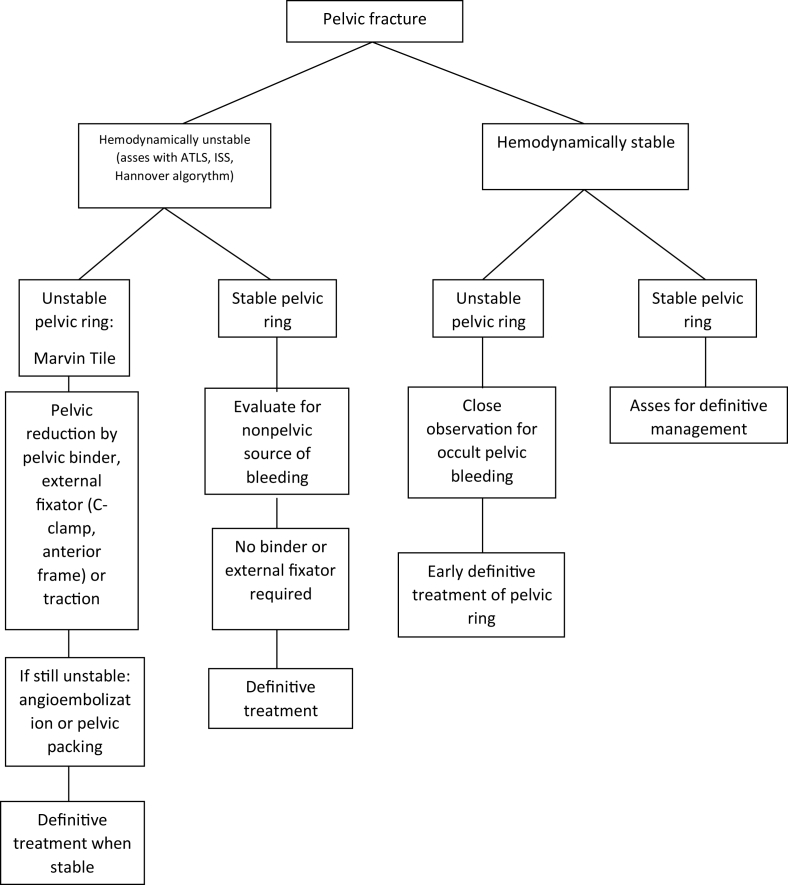
Presentation of case: Three cases of haemodynamically unstable pelvic fracture were studied retrospectively and prospectively. A staged approach using damage control orthopaedic surgery was performed. Initial resuscitation began from fluid resuscitation, pelvic wrapping using binder. All patients followed with pelvic external fixation, while 2 patients immediately replaced binder to C-Clamp, and 1 patient with anterior frame. Angioembolization was done to all patients. All patients required definitive internal fixation, while only 2 patients reach the definitive surgery. Finally, we measured the functional outcome of all patients using Hannover Pelvic score, Majeed pelvic score, and Iowa Pelvic score.
Discussion: We review some literatures regarding pelvic angioembolization. The previous study suggested to resuscitate patients when the hemodynamic is unstable, the angioembolization procedure is still preferred. The indication and successful definition of this procedure is still unclear, yet it shows decrease of mortality rate of pelvic injury if this procedure starts ahead a schedule.
Conclusion: Angioembolization as a part of damaged control orthopaedic has been shown a favorable result in managing unstable pelvic injury.
Keywords: Angiographic embolization; Pelvic fracture; Pelvic injury.
© 2021 The Authors.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures




Similar articles
-
Angioembolization provides benefits in patients with concomitant unstable pelvic fracture and unstable hemodynamics.Am J Emerg Med. 2012 Jan;30(1):207-13. doi: 10.1016/j.ajem.2010.11.005. Epub 2010 Dec 14. Am J Emerg Med. 2012. PMID: 21159470
-
The role of anterior supra-acetabular external fixator as definitive treatment for anterior ring fixation in unstable pelvic fractures.Eur J Trauma Emerg Surg. 2022 Oct;48(5):3737-3746. doi: 10.1007/s00068-021-01711-2. Epub 2021 Jun 7. Eur J Trauma Emerg Surg. 2022. PMID: 34097076
-
Retroperitoneal packing or angioembolization for haemorrhage control of pelvic fractures--Quasi-randomized clinical trial of 56 haemodynamically unstable patients with Injury Severity Score ≥33.Injury. 2016 Feb;47(2):395-401. doi: 10.1016/j.injury.2015.10.008. Epub 2015 Oct 22. Injury. 2016. PMID: 26508436 Clinical Trial.
-
Management of Hemodynamically Unstable Pelvic Ring Fractures.Front Surg. 2020 Dec 4;7:601321. doi: 10.3389/fsurg.2020.601321. eCollection 2020. Front Surg. 2020. PMID: 33425982 Free PMC article. Review.
-
Management of pelvic fractures.Curr Opin Crit Care. 2010 Dec;16(6):582-6. doi: 10.1097/MCC.0b013e3283402869. Curr Opin Crit Care. 2010. PMID: 20930625 Review.
Cited by
-
Effect of C-Clamp Application on Hemodynamic Instability in Polytrauma Victims with Pelvic Fracture.Medicina (Kaunas). 2022 Sep 16;58(9):1291. doi: 10.3390/medicina58091291. Medicina (Kaunas). 2022. PMID: 36143972 Free PMC article.
References
-
- Sarin E.L., Moore J.B., Moore E.E., Shannon M.R., Ray C.E., Morgan S.J. Pelvic fracture pattern does not always predict the need for urgent embolization. J. Trauma Inj. Infect. Crit. Care. 2005;58(5):973–977. - PubMed
-
- Tosounidis T.H., Sheikh H.Q., Kanakaris N.K., Giannoudis P.V. The use of external fixators in the definitive stabilisation of the pelvis in polytrauma patients: safety, efficacy and clinical outcomes. Injury. 2017;48(6):1139–1146. - PubMed
-
- Agha R.A., Sohrabi C., Mathew G., Franchi T., Kerwan A., O'Neill N. The PROCESS 2020 guideline: updating consensus preferred reporting of CasE series in surgery (PROCESS) guidelines. Int. J. Surg. 2020 Dec 1;84:231–235. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
