

Pretreatment Plasma EBV-DNA Load Guides Induction Chemotherapy Followed by Concurrent Chemoradiotherapy in Locoregionally Advanced Nasopharyngeal Cancer: A Meta-Analysis
- PMID: 33665166
- PMCID: PMC7921716
- DOI: 10.3389/fonc.2020.610787
Pretreatment Plasma EBV-DNA Load Guides Induction Chemotherapy Followed by Concurrent Chemoradiotherapy in Locoregionally Advanced Nasopharyngeal Cancer: A Meta-Analysis
Abstract
Background: The efficacy of induction chemotherapy (IC) followed by concurrent chemoradiotherapy (CCRT) in locoregionally advanced nasopharyngeal cancer (LA-NPC) is controversial. In this paper, we conduct a meta-analysis based on relevant studies to provide strong evidence for clinical strategies.
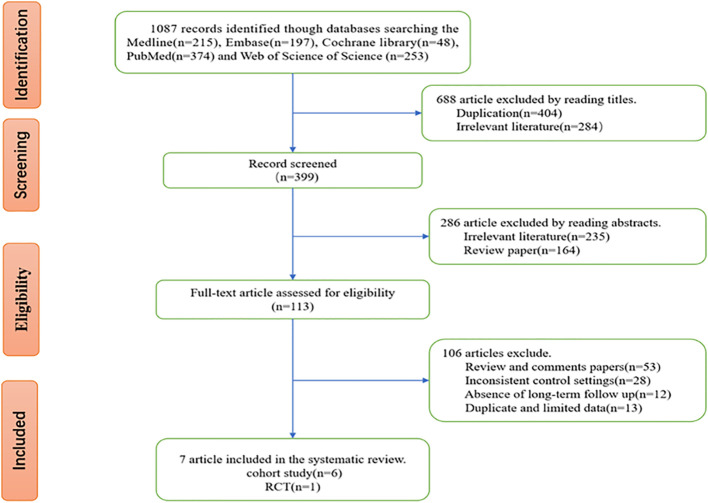
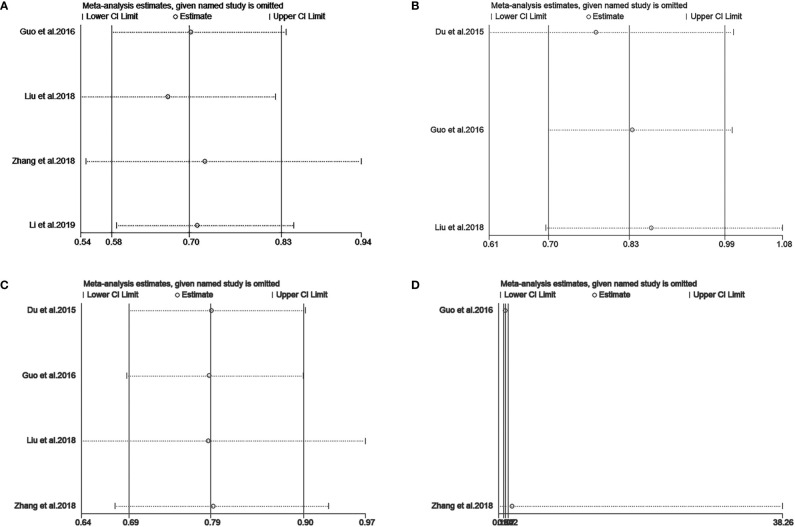
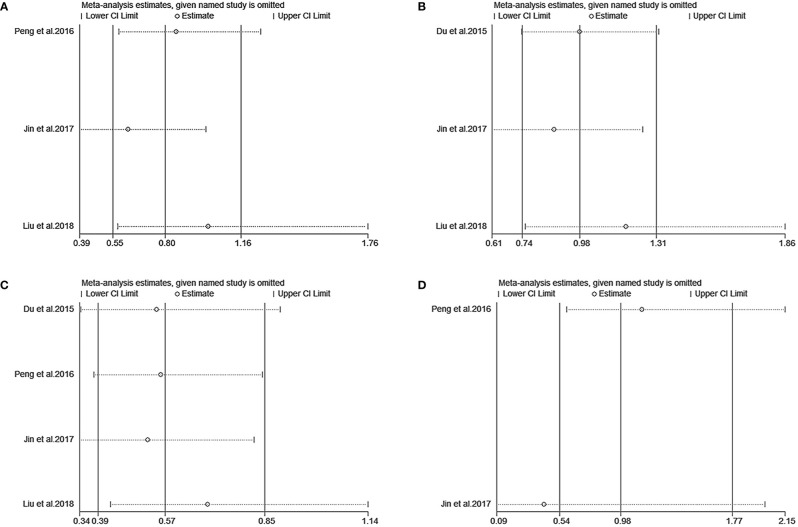
Materials and methods: We searched the MEDLINE, Embase, Cochrane, PubMed, and Web of Science databases for studies that stratified patients based on a high or low plasma Epstein-Barr virus deoxyribonucleic acid (EBV-DNA) load before treatment and compared the clinical efficacy of IC+CCRT vs. CCRT alone in LA-NPC. We tested for heterogeneity of studies and conducted sensitivity analysis. Subgroup analysis was performed for overall survival (OS), progression-free survival (PFS), distant metastasis-free survival (DMFS), and locoregional relapse-free survival (LRFS).
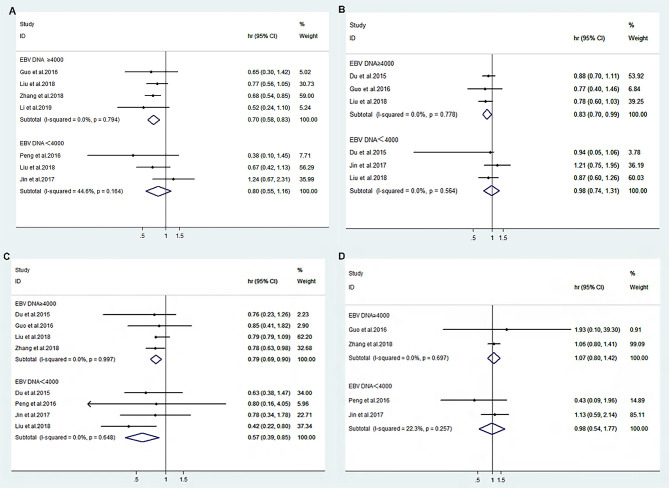
Results: Seven studies with a total of 5289 cases were finally included in the meta-analysis. The heterogeneity test revealed the homogeneity of OS (I 2 = 0.0%, p=0.794), PFS (I 2 = 0.0%, p=0.778), DMFS (I 2 = 0.0%, p=0.997), and LRFS (I 2 = 0.0%, p=0.697) in patients with EBV-DNA loads of ≥4000 copies/ml in both the IC+CCRT and CCRT groups. The results reveal that IC+CCRT significantly extended the OS (HR 0.70 [95% CI 0.58-0.83], p=0.000), PFS (HR 0.83 [95% CI 0.70-0.99], p=0.033), and DMFS (HR 0.79 [95% CI 0.69-0.9], p=0.000) of patients compared with the CCRT group, but there were no beneficial effects on LRFS (HR 1.07 [95% CI 0.80-1.42], p=0.647). The heterogeneity test found that there was no significant heterogeneity of PFS (I 2 = 0.0%, p=0.564), DMFS (I 2 = 0.0%, p=0.648), LRFS (I 2 = 22.3%, p=0.257), and OS (I 2 = 44.6%, p=0.164) in patients with EBV-DNA loads of <4000 copies/ml. The results show that IC+CCRT prolonged DMFS (HR 0.57 [95% CI 0.39-0.85], p=0.006) of patients without significant improvements in OS (HR 0.88 [95% CI 0.55-1.26], p=0.240), PFS (HR 0.98 [95% CI 0.74-1.31], p=0.908), and LRFS (HR 0.98 [95% CI 0.54-1.77], p=0.943).
Conclusions: Pretreatment plasma EBV-DNA can be considered a promising effective marker for the use of IC in LA-NPC patients. The addition of IC could improve the OS and PFS of patients with EBV-DNA load ≥4000 copies/ml, but we saw no efficacy in patients with EBV-DNA load <4000 copies/ml. Moreover, regardless of the EBV-DNA load, IC could improve DMFS, but there was no effect on LRFS.
Keywords: concurrent chemoradiotherapy; induction chemotherapy; locoregionally advanced nasopharyngeal cancer; meta-analysis; pretreatment plasma EBV-DNA load.
Copyright © 2021 Lai, Chen, Zhang, Chen, Chen, Tian and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lo YM, Chan AT, Chan LY, Leung SF, Lam CW, Huang DP, et al. Molecular prognostication of nasopharyngeal carcinoma by quantitative analysis of circulating Epstein-Barr virus DNA. Cancer Res (2000) 60(24):6878–81. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources