

Recurrent traumatic hip dislocation in an 8-year-old boy
- PMID: 33665312
- PMCID: PMC7900766
- DOI: 10.1016/j.tcr.2021.100418
Recurrent traumatic hip dislocation in an 8-year-old boy
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.Trauma Case Rep. 2023 Feb 17;45:100798. doi: 10.1016/j.tcr.2023.100798. eCollection 2023 Jun. Trauma Case Rep. 2023. PMID: 37234584 Free PMC article.
-
Erratum regarding missing Patient Consent statement in previously published articles.Trauma Case Rep. 2023 Mar 1;45:100818. doi: 10.1016/j.tcr.2023.100818. eCollection 2023 Jun. Trauma Case Rep. 2023. PMID: 37234590 Free PMC article.
Abstract
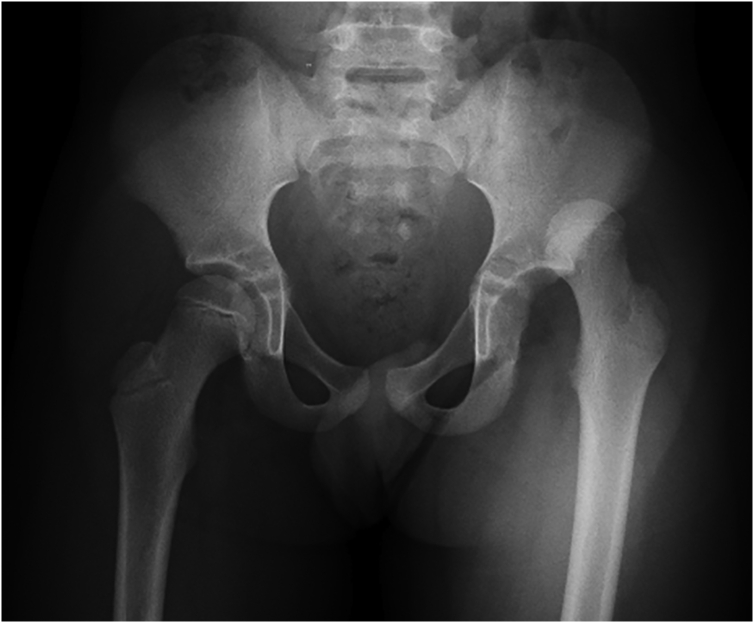
Pediatric traumatic hip dislocations (PTHD) are rare and represent around 5% of all pediatric dislocations. Associated bony or soft tissue injury can occur as often as 17%-25% of the time. We report a case of an 8-year-old boy presenting a posterior hip dislocation after a low-energy trauma, which was initially managed with closed reduction and bed rest for 1 week. Two days after hospital discharge, he suffered a recurrent posterior hip dislocation. He was now managed with 4 weeks of bed rest and lower limb skin traction followed by 1 week of no weight-bearing on crutches. With 6 months of follow-up, he is asymptomatic, walking autonomously, with complete and painless range of motion of the affected hip and no major radiographic changes. Pediatric traumatic hip dislocation is a rare and challenging injury that should be managed promptly. Currently, there is no protocol concerning treatment in the literature and its largely dependent of patient and parents' cooperation.
Keywords: Child; Closed reduction; Hip; Magnetic resonance imaging; Traumatic dislocation.
© 2021 The Authors.
Figures










References
-
- Stenroos A., Laaksonen T., Nietosvaara Y. Traumatic hip dislocation in pediatric patients. Duodecim; laaketieteellinen aikakauskirja. 2017;133(8):749–752. - PubMed
-
- Yuksel S., Albay C. Early reduction of pediatric traumatic posterior hip dislocation is much more important than the treatment procedure. Pediatr. Emerg. Care. 2019;35(11):e206–e208. - PubMed
-
- Hickerson L.E., Tuten H.R. Missed pediatric traumatic hip dislocation: a case report. JBJS Case Connector. 2013;3(1) - PubMed
-
- Basaran S.H., Bilgili M.G., Ercin E., Bayrak A., Ones H.N., Avkan M.C. Treatment and results in pediatric traumatic hip dislocation: case series and review of the literature. Ulusal travma ve acil cerrahi dergisi. 2014;20(6):437–442. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
