

Delay in ICU transfer is protective against ICU readmission in trauma patients: a naturally controlled experiment
- PMID: 33665369
- PMCID: PMC7893658
- DOI: 10.1136/tsaco-2021-000695
Delay in ICU transfer is protective against ICU readmission in trauma patients: a naturally controlled experiment
Abstract
Background: Unplanned intensive care unit (ICU) readmission-ICU bounce back (ICUbb)-is associated with worse outcomes. Patients not requiring organ system support or intensive nursing are deemed 'ICU discharge ready' and transfer orders are placed. However, actual transfer only occurs when an appropriate, non-ICU bed is available. This is dependent on inherent system inefficiencies resulting in a naturally controlled experiment between when patients actually transfer: Early (<24 hours) or Delayed (>24 hours) transfers, after order placement. This study leverages that natural experiment to determine if additional ICU time is protective against ICUbb. We hypothesize that Delayed transfer is protective against ICUbb.
Methods: Using a retrospective, cohort design, we queried a trauma research repository and electronic medical record during a 10-year period to capture traumatized patients admitted to the ICU. Patients were categorized into Early (<24 hours) or Unintended-Delayed (>24 hours) groups based on actual transfer time after order placement. Patient characteristics (age, Charlson Comorbidity Index (CCI)) and Injury Severity Score (ISS) were analyzed. Univariate and multivariate analyses were performed to compare ICUbb rates among Early and Unintended-Delayed groups.
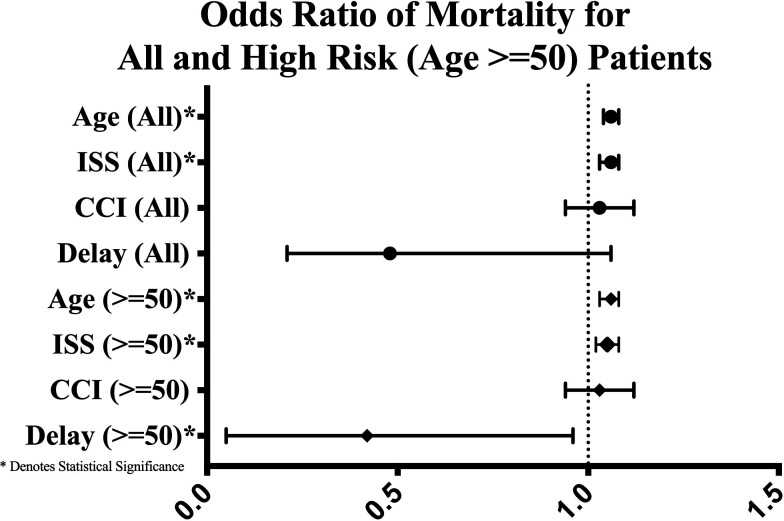
Results: Of the 2004 patients who met the criteria, 1690 fell into the Early group, and 314 fell into the Delayed. The Early group was younger (mean age 52±23 vs. 55±22 years), had fewer comorbidities (median CCI score 1 (0, 3) vs. 2 (1, 3)), and was less injured (median ISS 17 (10-22) vs. 17 (13-25)), all p<0.05. Overall, 113 (5.6%) patients experienced ICUbb: Early 109 (6.5%) versus Unintended-Delay 4 (1.3%), p<0.05. By regression analysis, age, CCI, and ISS were independently associated with ICUbb while Delayed transfer was protective.
Discussion: Despite higher age, CCI score, and ISS, the Unintended-Delayed group experienced fewer ICUbb. After controlling for age, CCI and ISS, Delayed transfer reduced ICUbb risk by 78%. Specific care elements affording this protection remain to be elucidated.
Level of evidence: Level III.
Study type: Therapeutic study.
Keywords: intensive care units; multiple trauma; patient readmission; quality improvement.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Litwinowicz R, Bartus K, Drwila R, Kapelak B, Konstanty-Kalandyk J, Sobczynski R, Wierzbicki K, Bartuś M, Chrapusta A, Timek T, et al. In-Hospital mortality in cardiac surgery patients after readmission to the intensive care unit: a single-center experience with 10,992 patients. J Cardiothorac Vasc Anesth 2015;29:570–5. 10.1053/j.jvca.2015.01.029 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous