

Effect of preoperative long-term opioid therapy on patient outcomes after total knee arthroplasty: an analysis of multicentre population-based administrative data
- PMID: 33666382
- PMCID: PMC8064248
- DOI: 10.1503/cjs.007319
Effect of preoperative long-term opioid therapy on patient outcomes after total knee arthroplasty: an analysis of multicentre population-based administrative data
Abstract
Background: Up to 40% of patients are receiving opioids at the time of total knee arthroplasty (TKA) in the United States despite evidence suggesting opioids are ineffective for pain associated with arthritis and have substantial risks. Our primary objective was to determine whether preoperative opioid users had worse knee pain and physical function outcomes 12 months after TKA than patients who were opioid-naive preoperatively; our secondary objective was to determine the prevalence of opioid use before and after TKA in Alberta, Canada.
Methods: In this retrospective analysis of population-based data, we identified adult patients who underwent TKA between 2013 and 2015 in Alberta. We used multivariable linear regression to examine the association between preoperative opioid use and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and physical function scores 12 months after TKA, adjusting for potentially confounding variables.
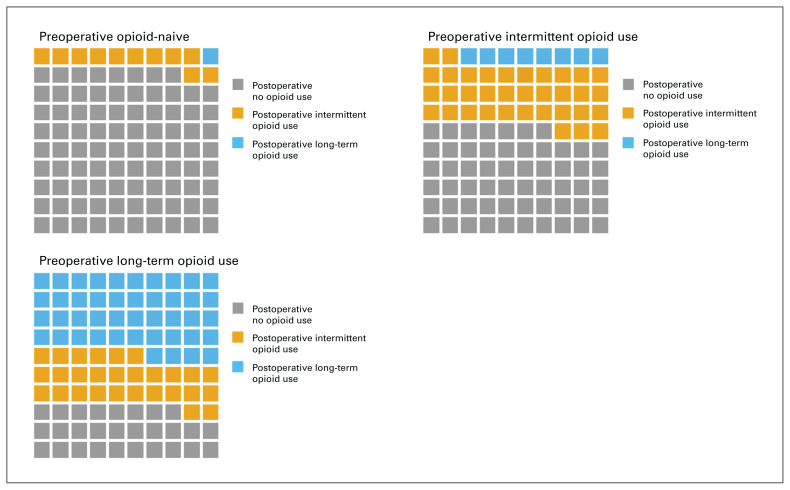
Results: Of the 1907 patients, 592 (31.0%) had at least 1 opioid dispensed before TKA, and 124 (6.5%) were classified as long-term opioid users. Long-term opioid users had worse adjusted WOMAC pain and physical function scores 12 months after TKA than patients who were opioid-naive preoperatively (pain score β = 7.7, 95% confidence interval [CI] 4.0 to 11.6; physical function score β = 7.8, 95% CI 4.0 to 11.6; p < 0.001 for both). The majority (89 ([71.8%]) of patients who were long-term opioid users preoperatively were dispensed opioids 180-360 days after TKA, compared to 158 (12.0%) patients who were opioid-naive preoperatively.
Conclusion: A substantial number of patients were dispensed opioids before and after TKA, and patients who received opioids preoperatively had worse adjusted pain and functional outcome scores 12 months after TKA than patients who were opioidnaive preoperatively. These results suggest that patients prescribed opioids preoperatively should be counselled judiciously regarding expected outcomes after TKA.
Contexte: Jusqu’à 40 % des patients se font prescrire des opioïdes lors d’une chirurgie pour prothèse totale du genou (PTG) aux États-Unis, et ce, malgré des données selon lesquelles les opioïdes sont inefficaces pour la douleur associée à l’arthrite et comportent des risques substantiels. Notre objectif principal était de déterminer si les patients qui utilisaient déjà des opioïdes en période préopératoire obtenaient des résultats plus négatifs aux plans de la douleur et du fonctionnement 12 mois après leur PTG, comparativement aux patients qui ne prenaient pas d’opioïdes avant leur intervention; notre objectif secondaire était de mesurer la prévalence du recours aux opioïdes avant et après la PTG en Alberta, au Canada.
Méthodes: Dans cette analyse rétrospective menée sur des données de population, nous avons identifié les patients adultes soumis à une PTG entre 2013 et 2015 en Alberta. Nous avons utilisé un modèle de régression linéaire multivarié pour examiner le lien entre l’utilisation d’opioïdes en période préopératoire et les scores de douleur et de fonctionnement à l’échelle WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) 12 mois après la PTG, en tenant compte de potentielles variables de confusion.
Résultats: Sur les 1907 patients, 592 (31,0 %) ont reçu au moins 1 opioïde avant leur PTG, et 124 (6,5 %) en étaient considérés des utilisateurs de longue date. Les utilisateurs d’opioïdes de longue date présentaient de moins bons scores WOMAC ajustés pour les domaines de douleur et de fonctionnement 12 mois après la PTG, comparativement aux patients qui n’en prenaient pas avant l’intervention (score de douleur β = 7,7, intervalle de confiance [IC] de 95 % 4,0 à 11,6; score de fonctionnement β = 7,8, IC de 95 % 4,0 à 11,6; p < 0,001 pour les 2 domaines). La majorité (89 [71,8 %]) des patients utilisateurs d’opioïdes de longue date avant l’intervention se sont fait servir des opioïdes 180–360 jours après la PTG, comparativement à 158 patients (12,0 %) qui n’en prenaient pas avant l’intervention.
Conclusion: Un nombre substantiel de patients ont reçu des opioïdes avant et après la PTG, et ceux qui en prenaient avant l’intervention présentaient des scores de douleur et de fonctionnement ajustés plus défavorables 12 mois après la PTG, comparativement aux patients qui n’en prenaient pas avant l’intervention. Selon ces résultats, il faut adresser des conseils judicieux aux patients qui sont déjà sous opioïdes en période préopératoire et les informer des résultats possibles de la PTG.
© 2021 Joule Inc. or its licensors.
Conflict of interest statement
None declared.
Figures

References
-
- Busse JW, editor. The 2017 Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Hamilton (ON): National Pain Centre, McMaster University; 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical