

Outcome of the frozen elephant trunk procedure as a redo operation
- PMID: 33667306
- PMCID: PMC8923373
- DOI: 10.1093/icvts/ivab059
Outcome of the frozen elephant trunk procedure as a redo operation
Abstract
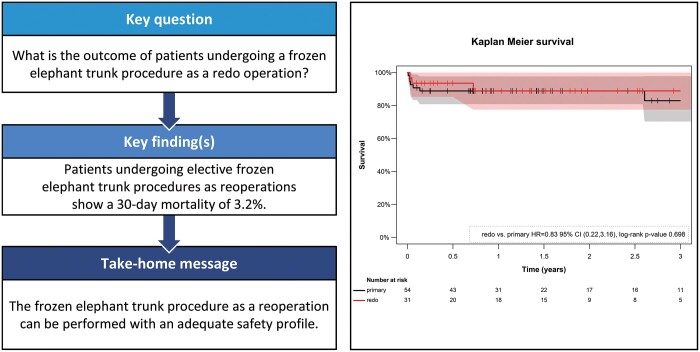
Objectives: The goal of this study was to determine the outcome of patients undergoing an elective frozen elephant trunk (FET) procedure as a redo operation following previous cardiac surgery.
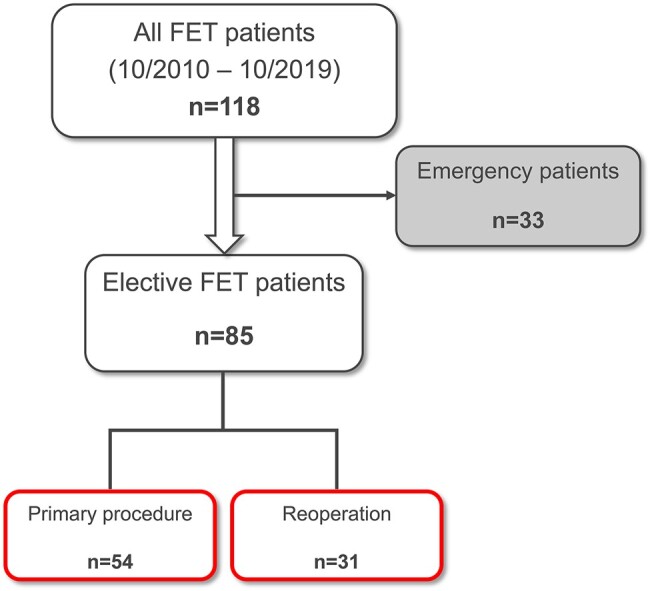
Methods: One hundred and eighteen consecutive patients underwent FET procedures between October 2010 and October 2019 at our centre. Patients were registered in a dedicated database and analysed retrospectively. Clinical and follow-up characteristics were compared between patients undergoing a FET operation as a primary (primary group) or a redo procedure (redo group) using logistic regression and Cox regression analysis. Emergency procedures (n = 33) were excluded from the analysis.
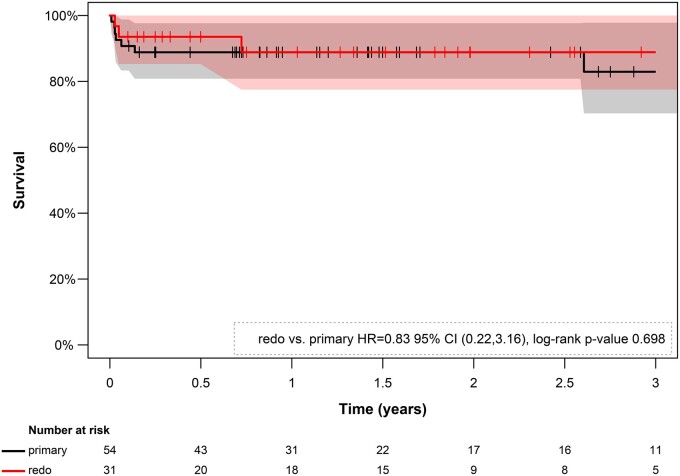
Results: A total of 36.5% (n = 31) of the FET procedures were redo operations (redo group) and 63.5% (n = 54) of the patients underwent primary surgery (primary group). There was no significant difference in the 30-day mortality [primary group: 7.4%; redo group: 3.2%; 95% confidence interval (CI) (0.19-35.29); P = 0.63] and the 3-year mortality [primary group: 22.2%; redo group: 16.7%; 95% CI (0.23-3.23); P = 0.72] between redo and primary cases. Furthermore, the adjusted statistical analysis did not reveal significant differences between the groups in the occurrence of transient or permanent neurological deficit, paraplegia, acute renal failure and resternotomy. The redo group showed a higher rate of recurrent nerve palsy, which did not reach statistical significance [primary group: 3.7% (n = 2); redo group: 19.4% (n = 6); P = 0.091].
Conclusions: Elective FET procedures as redo operations performed by a dedicated aortic team following previous cardiac surgery demonstrate an adequate safety profile.
Keywords: Aortic aneurysm; Aortic arch replacement; Endovascular procedures; Frozen elephant trunk; Reoperation.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
Similar articles
-
Experience with the conventional and frozen elephant trunk techniques: a single-centre study.Eur J Cardiothorac Surg. 2013 Dec;44(6):1076-82; discussion 1083. doi: 10.1093/ejcts/ezt252. Epub 2013 May 15. Eur J Cardiothorac Surg. 2013. PMID: 23677901
-
Is the frozen elephant trunk procedure superior to the conventional elephant trunk procedure for completion of the second stage?Eur J Cardiothorac Surg. 2017 Oct 1;52(4):725-732. doi: 10.1093/ejcts/ezx199. Eur J Cardiothorac Surg. 2017. PMID: 28655150
-
Conventional versus frozen elephant trunk surgery for extensive disease of the thoracic aorta.J Cardiovasc Med (Hagerstown). 2014 Nov;15(11):803-9. doi: 10.2459/JCM.0b013e328364559c. J Cardiovasc Med (Hagerstown). 2014. PMID: 23867913
-
"Proximalization is Advancement"-Zone 3 Frozen Elephant Trunk vs Zone 2 Frozen Elephant Trunk: A Literature Review.Vasc Endovascular Surg. 2021 Aug;55(6):612-618. doi: 10.1177/15385744211002493. Epub 2021 Mar 23. Vasc Endovascular Surg. 2021. PMID: 33754903 Review.
-
Review of frozen elephant trunk repair with the Thoraflex Hybrid device.Future Cardiol. 2021 Oct;17(7):1171-1181. doi: 10.2217/fca-2020-0152. Epub 2021 Feb 5. Future Cardiol. 2021. PMID: 33544641 Review.
Cited by
-
Mid-term morphological changes in Frozenix.Interdiscip Cardiovasc Thorac Surg. 2025 May 6;40(5):ivaf104. doi: 10.1093/icvts/ivaf104. Interdiscip Cardiovasc Thorac Surg. 2025. PMID: 40341351 Free PMC article.
-
Surgical Strategies in Reoperation of the Proximal Aorta and Arch for Patients with Previous Frozen Elephant Trunk.J Clin Med. 2024 Jul 11;13(14):4063. doi: 10.3390/jcm13144063. J Clin Med. 2024. PMID: 39064105 Free PMC article.
-
Reintervention of Residual Aortic Dissection after Type A Aortic Repair: Results of a Prospective Follow-Up at 5 Years.J Clin Med. 2023 Mar 18;12(6):2363. doi: 10.3390/jcm12062363. J Clin Med. 2023. PMID: 36983363 Free PMC article.
-
Complicated acute type A aortic dissection and severe aortic atherosclerosis predict early mortality after frozen elephant trunk procedure.Eur J Cardiothorac Surg. 2025 Jul 1;67(7):ezaf213. doi: 10.1093/ejcts/ezaf213. Eur J Cardiothorac Surg. 2025. PMID: 40576437 Free PMC article.
-
Analysing debranching techniques in Frozen Elephant Trunk procedures: a narrative literature review.Cardiovasc Diagn Ther. 2023 Apr 28;13(2):427-439. doi: 10.21037/cdt-22-502. Epub 2023 Mar 22. Cardiovasc Diagn Ther. 2023. PMID: 37583690 Free PMC article. Review.
References
-
- Leontyev S, Tsagakis K, Pacini D, Di Bartolomeo R, Mohr FW, Weiss G. et al. Impact of clinical factors and surgical techniques on early outcome of patients treated with frozen elephant trunk technique by using EVITA open stent-graft: results of a multicentre study. Eur J Cardiothorac Surg 2016;49:660–6. - PubMed
-
- Parikh N, Trimarchi S, Gleason TG, Kamman AV, di Eusanio M, Myrmel T. et al. Changes in operative strategy for patients enrolled in the International Registry of Acute Aortic Dissection interventional cohort program. J Thorac Cardiovasc Surg 2017;153:S74–79. - PubMed
-
- Geirsson A, Bavaria JE, Swarr D, Keane MG, Woo YJ, Szeto WY. et al. Fate of the residual distal and proximal aorta after acute type A dissection repair using a contemporary surgical reconstruction algorithm. Ann Thorac Surg 2007;84:1955–64. - PubMed
-
- Detter C, Demal TJ, Bax L, Tsilimparis N, Kölbel T, von Kodolitsch Y. et al. Simplified frozen elephant trunk technique for combined open and endovascular treatment of extensive aortic diseases. Eur J Cardiothorac Surg 2019;56:738–45. - PubMed
-
- Bender R, Lange S.. Adjusting for multiple testing—when and how? J Clin Epidemiol 2001;54:343–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
