

The Global Burden of Meningitis in Children: Challenges with Interpreting Global Health Estimates
- PMID: 33668442
- PMCID: PMC7917636
- DOI: 10.3390/microorganisms9020377
The Global Burden of Meningitis in Children: Challenges with Interpreting Global Health Estimates
Abstract
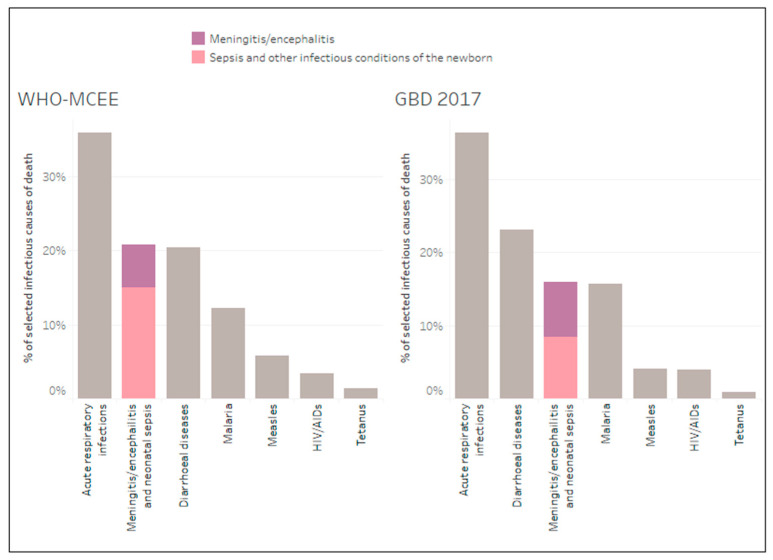
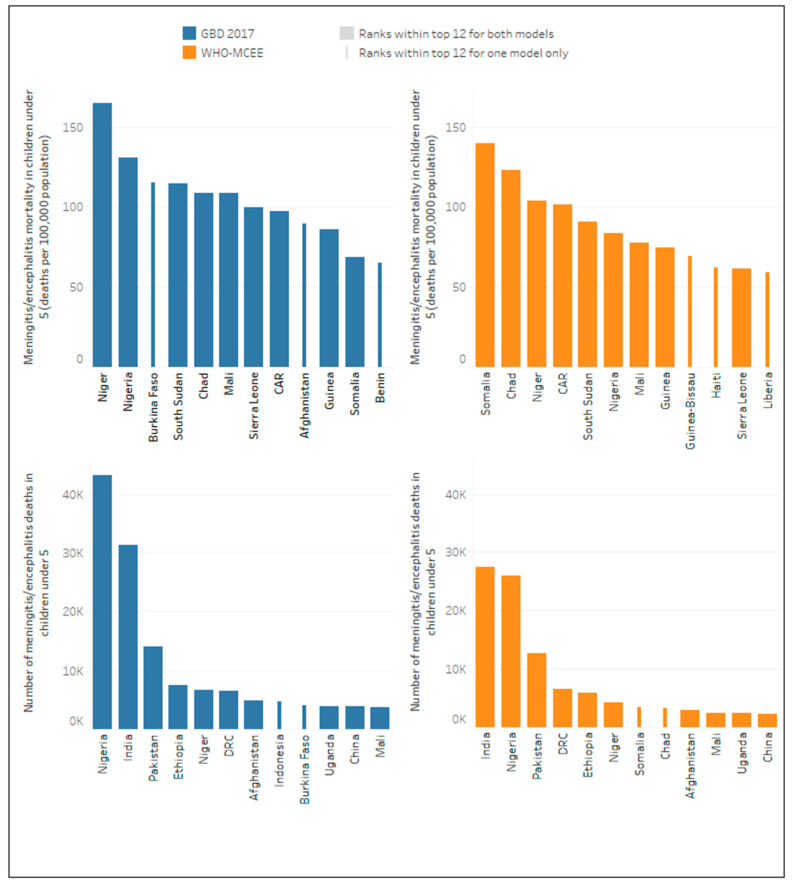
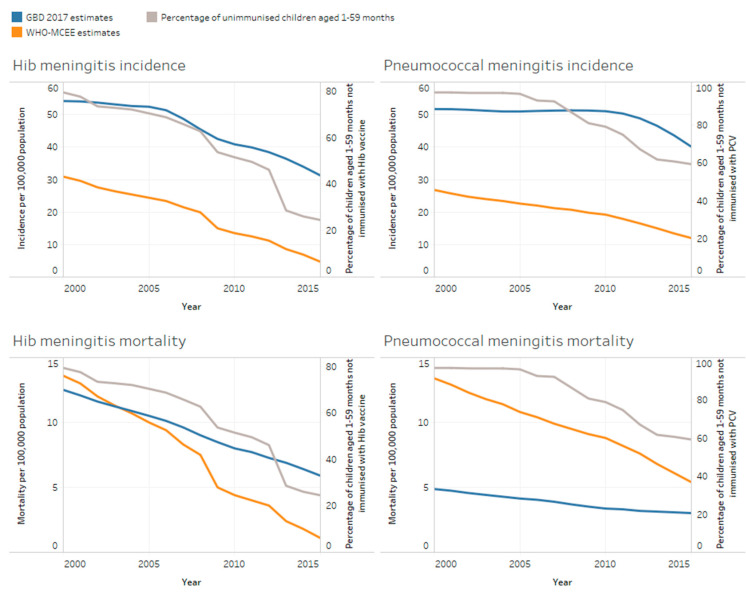
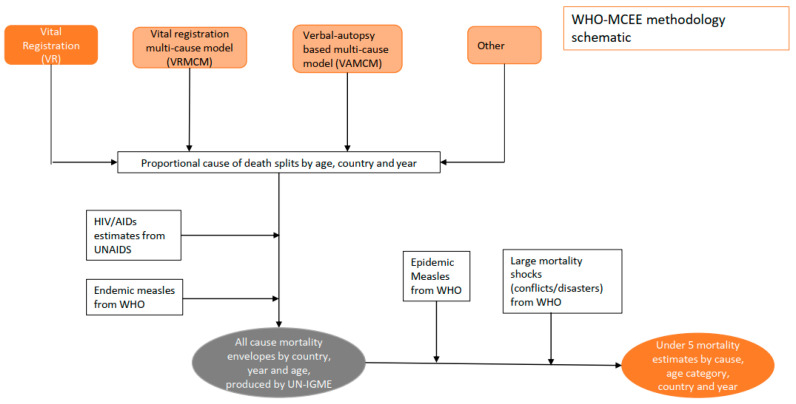
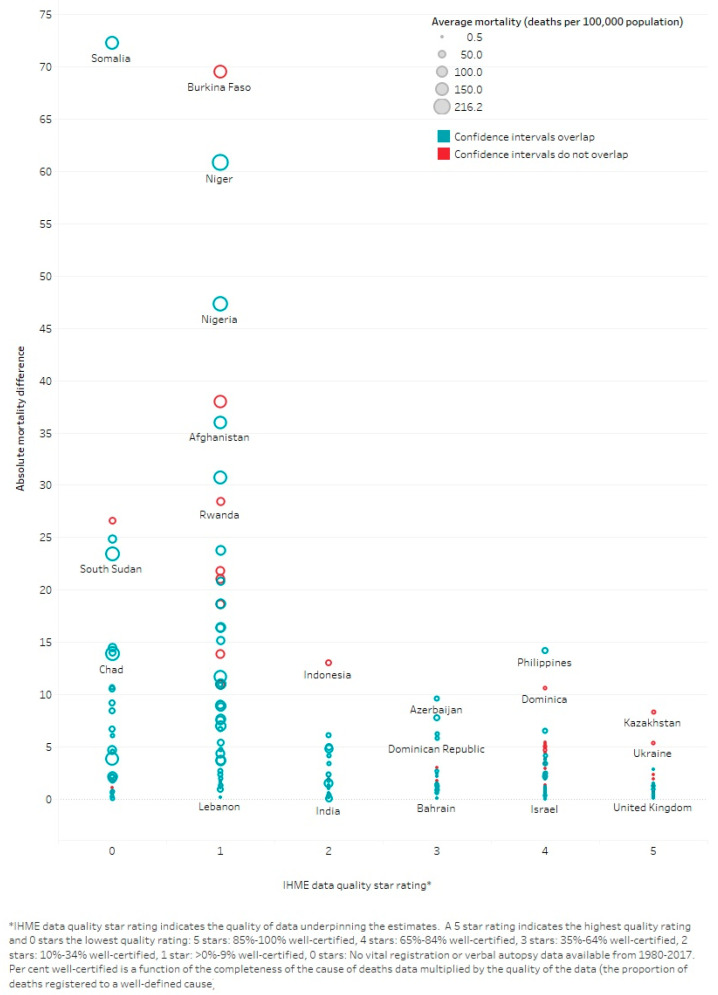
The World Health Organization (WHO) has developed a global roadmap to defeat meningitis by 2030. To advocate for and track progress of the roadmap, the burden of meningitis as a syndrome and by pathogen must be accurately defined. Three major global health models estimating meningitis mortality as a syndrome and/or by causative pathogen were identified and compared for the baseline year 2015. Two models, (1) the WHO and the Johns Hopkins Bloomberg School of Public Health's Maternal and Child Epidemiology Estimation (MCEE) group's Child Mortality Estimation (WHO-MCEE) and (2) the Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease Study (GBD 2017), identified meningitis, encephalitis and neonatal sepsis, collectively, to be the second and third largest infectious killers of children under five years, respectively. Global meningitis/encephalitis and neonatal sepsis mortality estimates differed more substantially between models than mortality estimates for selected infectious causes of death and all causes of death combined. Estimates at national level and by pathogen also differed markedly between models. Aligning modelled estimates with additional data sources, such as national or sentinel surveillance, could more accurately define the global burden of meningitis and help track progress against the WHO roadmap.
Keywords: Haemophilus influenzae; Neisseria meningitidis; Streptococcus pneumoniae; child mortality; global health; global health estimates; meningitis; modelling; neonatal sepsis.
Conflict of interest statement
C.T. received a consulting payment from GSK in 2018 outside the submitted work. C.W., N.B., L.G., V.S. took part in this research as employees of Meningitis Research Foundation, which has received unrestricted educational grants from GSK, Pfizer and Sanofi. All other authors declare no conflict of interest. GSK, Pfizer and Sanofi had no role in the design of this study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) Levels & Trends in Child Mortality: Report 2020, Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation. [(accessed on 1 December 2020)];2020 Available online: https://www.un.org/development/desa/pd/news/levels-and-trends-child-mort....
-
- Zunt J.R., Kassebaum N.J., Blake N., Glennie L., Wright C., Nichols E., Abd-Allah F., Abdela J., Abdelalim A., A Adamu A., et al. Global, regional, and national burden of meningitis, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17:1061–1082. doi: 10.1016/S1474-4422(18)30387-9. - DOI - PMC - PubMed
-
- GBD Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- World Health Organization Global Action Plan on Antimicrobial Resistance. [(accessed on 3 February 2020)]; Available online: https://www.who.int/antimicrobial-resistance/publications/global-action-...
-
- Global Strategy for Women’s, Children’s, and Adolescents’ Health 2016–2030. [(accessed on 3 February 2020)]; Available online: https://www.who.int/life-course/partners/global-strategy/globalstrategyr....
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
