

Uremic Toxins in the Progression of Chronic Kidney Disease and Cardiovascular Disease: Mechanisms and Therapeutic Targets
- PMID: 33668632
- PMCID: PMC7917723
- DOI: 10.3390/toxins13020142
Uremic Toxins in the Progression of Chronic Kidney Disease and Cardiovascular Disease: Mechanisms and Therapeutic Targets
Abstract
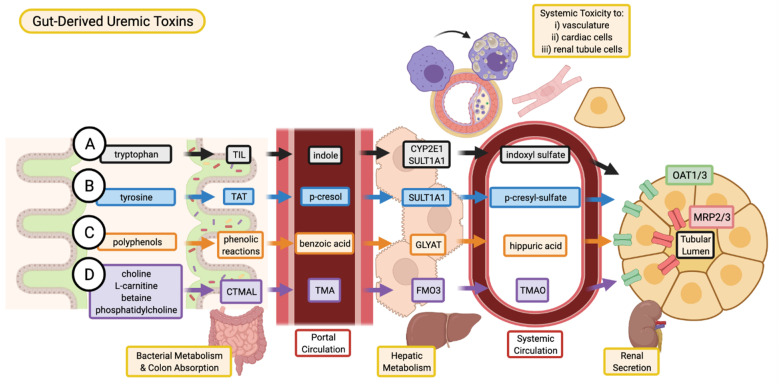
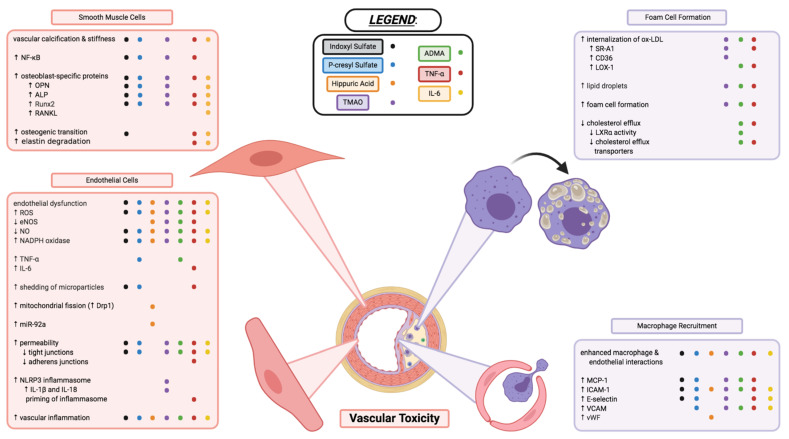
Chronic kidney disease (CKD) is a progressive loss of renal function. The gradual decline in kidney function leads to an accumulation of toxins normally cleared by the kidneys, resulting in uremia. Uremic toxins are classified into three categories: free water-soluble low-molecular-weight solutes, protein-bound solutes, and middle molecules. CKD patients have increased risk of developing cardiovascular disease (CVD), due to an assortment of CKD-specific risk factors. The accumulation of uremic toxins in the circulation and in tissues is associated with the progression of CKD and its co-morbidities, including CVD. Although numerous uremic toxins have been identified to date and many of them are believed to play a role in the progression of CKD and CVD, very few toxins have been extensively studied. The pathophysiological mechanisms of uremic toxins must be investigated further for a better understanding of their roles in disease progression and to develop therapeutic interventions against uremic toxicity. This review discusses the renal and cardiovascular toxicity of uremic toxins indoxyl sulfate, p-cresyl sulfate, hippuric acid, TMAO, ADMA, TNF-α, and IL-6. A focus is also placed on potential therapeutic targets against uremic toxicity.
Keywords: asymmetric dimethylarginine; cardiovascular disease; chronic kidney disease; hippuric acid; indoxyl sulfate; interleukin 6; p-cresyl sulfate; trimethylamine N-oxide; tumor necrosis factor al-pha; uremic toxins.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013;3:1–150.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
