

Intensity of Respiratory Cortical Arousals Is a Distinct Pathophysiologic Feature and Is Associated with Disease Severity in Obstructive Sleep Apnea Patients
- PMID: 33668974
- PMCID: PMC7996607
- DOI: 10.3390/brainsci11030282
Intensity of Respiratory Cortical Arousals Is a Distinct Pathophysiologic Feature and Is Associated with Disease Severity in Obstructive Sleep Apnea Patients
Abstract
Background: We investigated whether the number, duration and intensity of respiratory arousals (RA) on C3-electroencephalographic (EEG) recordings correlate with polysomnography (PSG)-related disease severity in obstructive sleep apnea (OSA) patients. We also investigated if every patient might have an individual RA microstructure pattern, independent from OSA-severity.
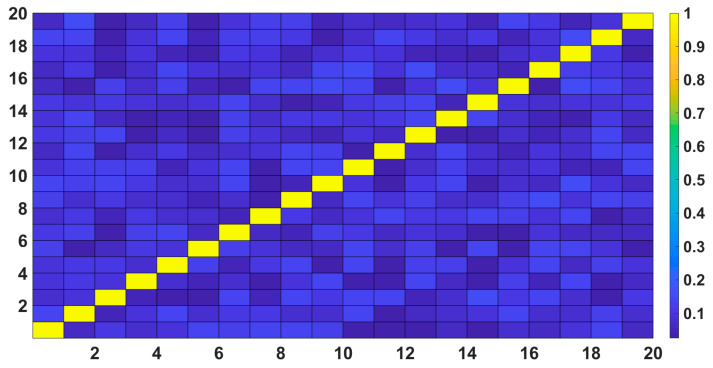
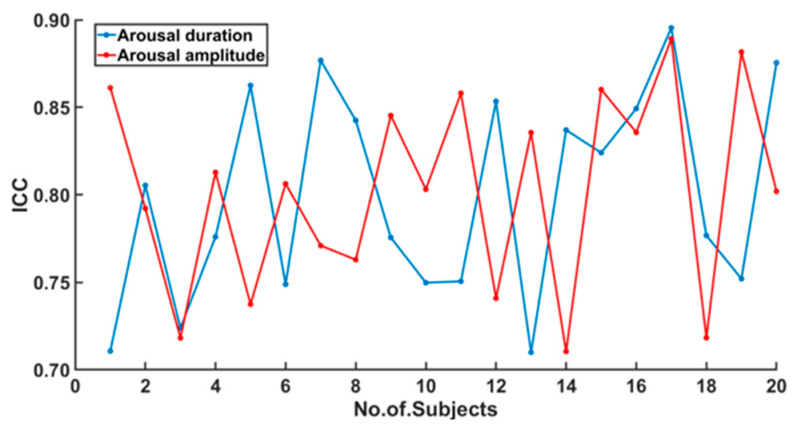
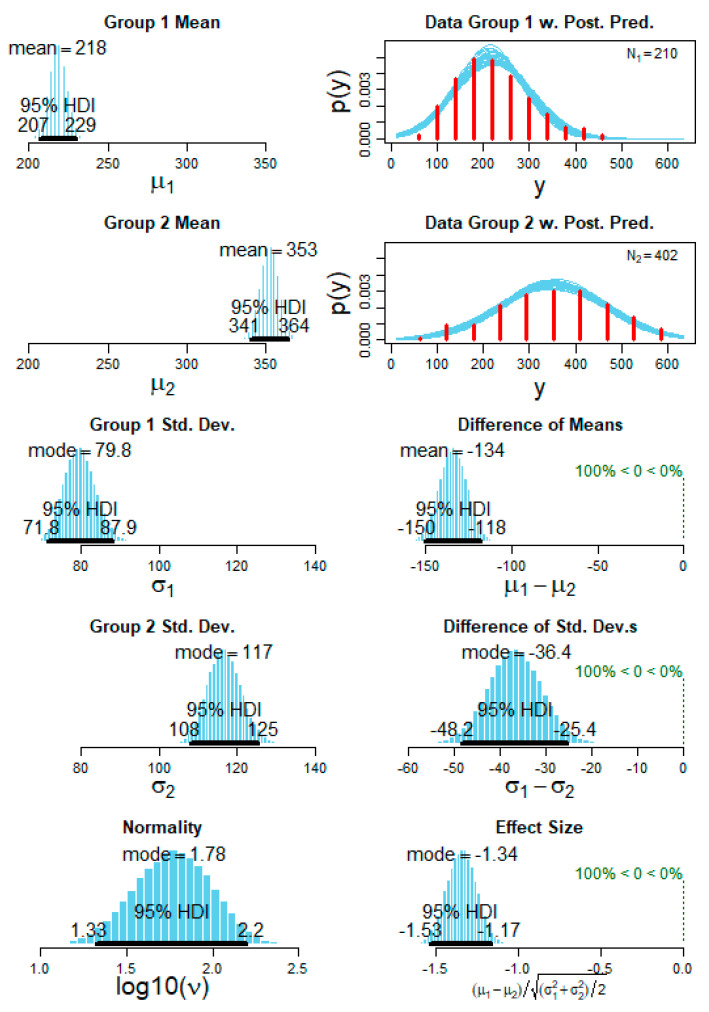
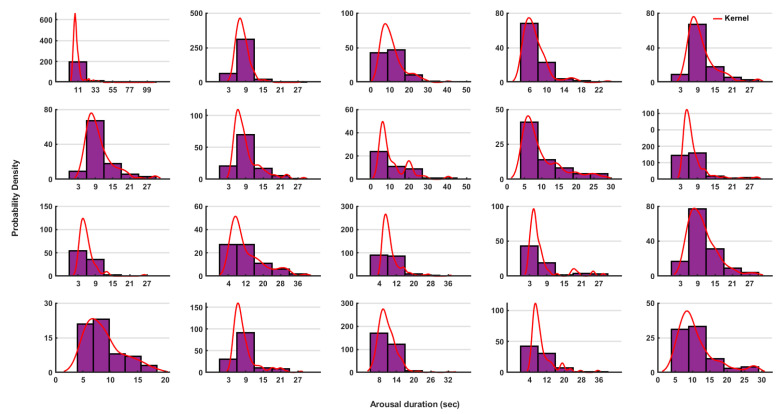
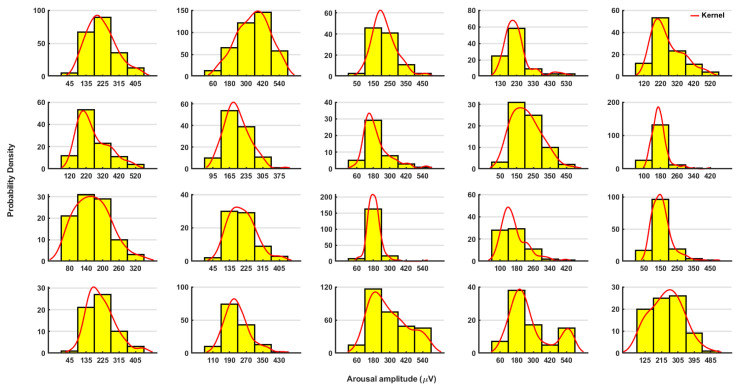
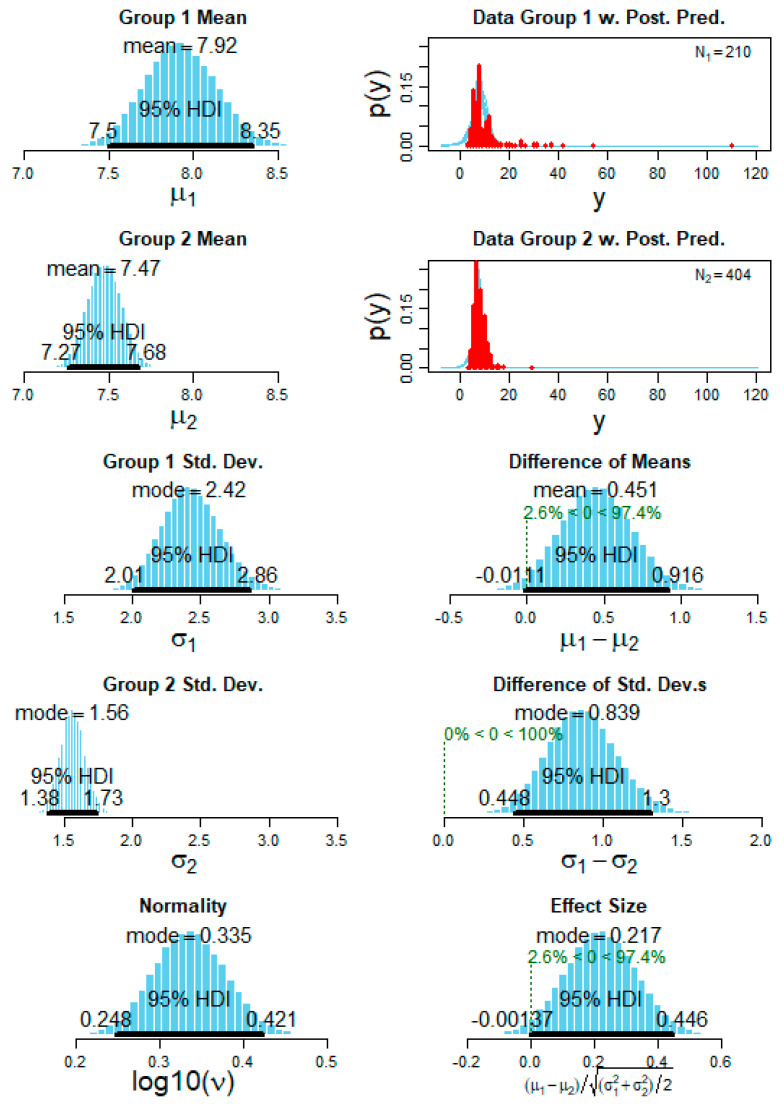
Methods: PSG recordings of 20 OSA patients (9 female; age 27-80 years) were analyzed retrospectively. Correlation coefficients were calculated between RA microstructure (duration, EEG-intensity) and RA number and respiratory disturbance index (RDI), oxygen desaturation index (ODI) and arousal index (AI). Intraclass correlations (ICC) for both RA duration and intensity were calculated. Sleep stage-specific and apnea- and hypopnea-specific analyses were also done. The probability distributions of duration and intensity were plotted, interpolated with a kernel which fits the distribution. A Bayesian posterior distribution analysis and pair-wise comparisons of each patient with all other 19 patients were performed.
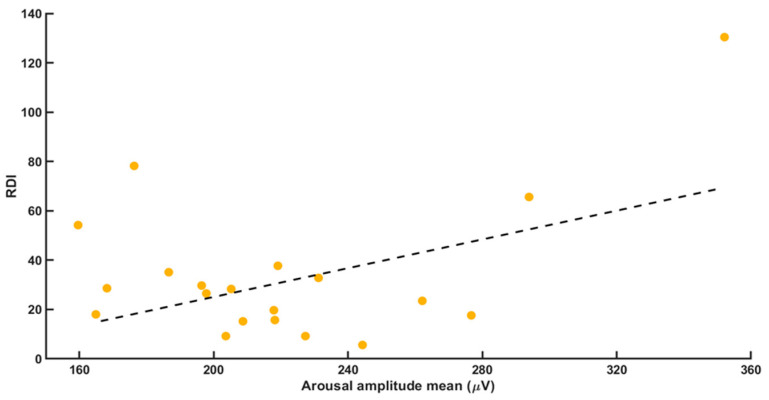
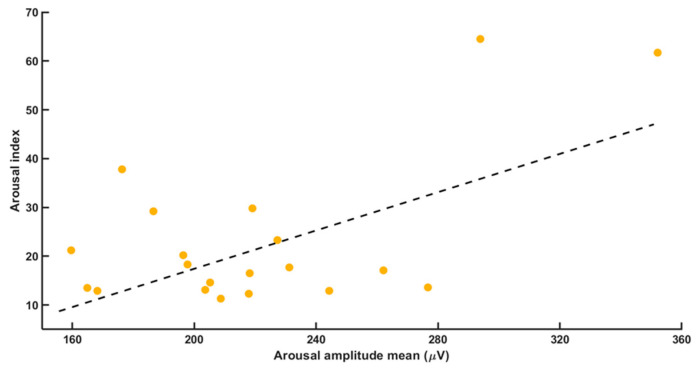
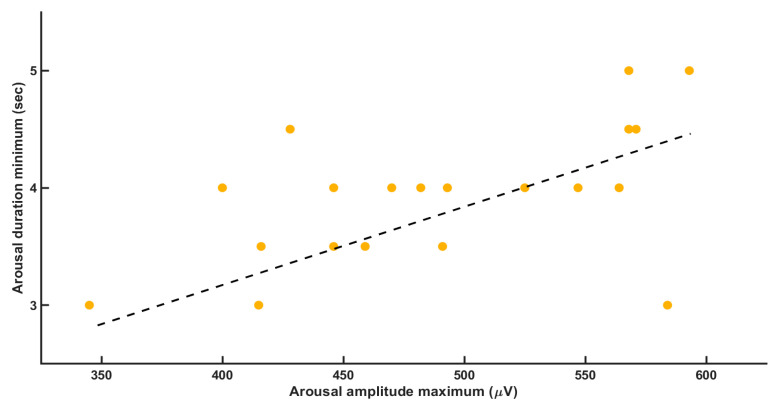
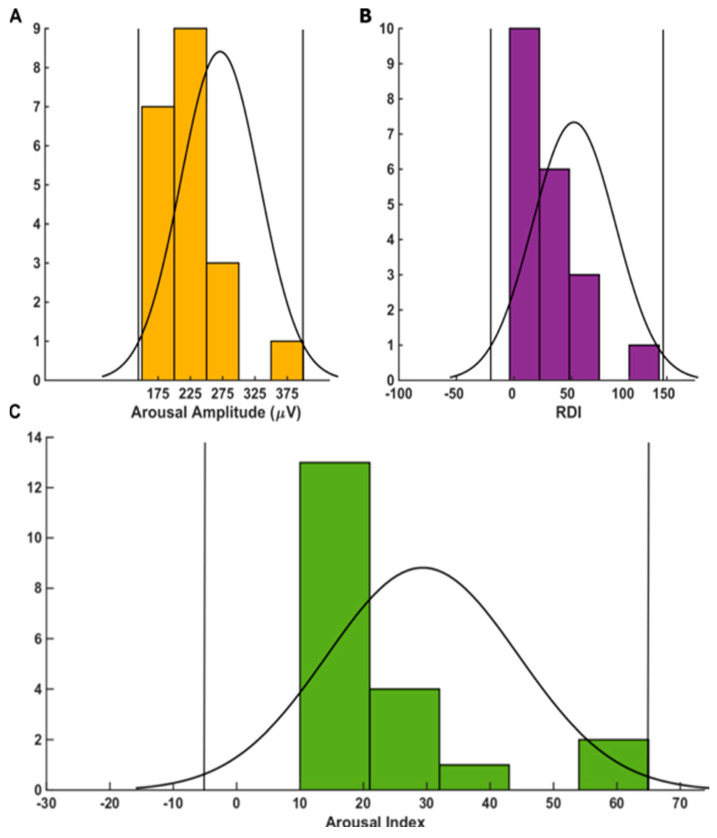
Results: Of the analyzed 2600 RA, strong positive correlations were found between average RA intensity and both RDI and AI. The number of PSG-recorded RA was strongly positively correlated with RDI. Significant correlations between average RA intensity in REM, NREM2 and NREM3 sleep stages and total ODI were identified. No sleep stage-specific correlations of arousal microstructure with age, sex, RDI or AI were identified. Although between-subjects ICC values were <0.25, within-subject ICC values were all >0.7 (all p < 0.05). While apnea-related RA duration did not differ from hypopnea-related RA duration, RA intensity was significantly higher (p = 0.00135) in hypopneas than in apneas. A clear individual pattern of arousal duration for each patient was made distinct. For arousal intensity, a Gaussian distribution was identified in most patients. The Bayesian statistics regarding the arousal microstructure showed significant differences between each pair of patients.
Conclusions: Each individual patient with OSA might have an individual pattern of RA intensity and duration indicating a distinct individual pathophysiological feature. Arousal intensity was significantly higher in hypopneic than in apneic events and may be related causally to the diminished (compared to apneas) respiratory distress associated with hypopneas. RA intensity in REM, NREM2 and NREM3 strongly correlated with ODI.
Keywords: arousal; microstructure; respiratory; sleep apnea; sleep-disturbed breathing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Berry R., Brooks R., Gamaldo C., Harding S.M., Lloyd R.M., Marcus C.L., Vaughn B.V. AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. American Academy of Sleep Medicine; Darien, IL, USA: 2007.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
