

Comparison of Immunogenicity and Safety between a Single Dose and One Booster Trivalent Inactivated Influenza Vaccination in Patients with Chronic Kidney Disease: A 20-Week, Open-Label Trial
- PMID: 33669067
- PMCID: PMC7996510
- DOI: 10.3390/vaccines9030192
Comparison of Immunogenicity and Safety between a Single Dose and One Booster Trivalent Inactivated Influenza Vaccination in Patients with Chronic Kidney Disease: A 20-Week, Open-Label Trial
Abstract
Background: Non-dialysis-dependent chronic kidney disease (CKD-ND) patients are recommended to receive a one-dose influenza vaccination annually. However, studies investigating vaccine efficacy in the CKD-ND population are still lacking. In this study, we aimed to evaluate vaccine efficacy between the one-dose and two-dose regimen and among patients with different stages of CKD throughout a 20-week follow-up period.
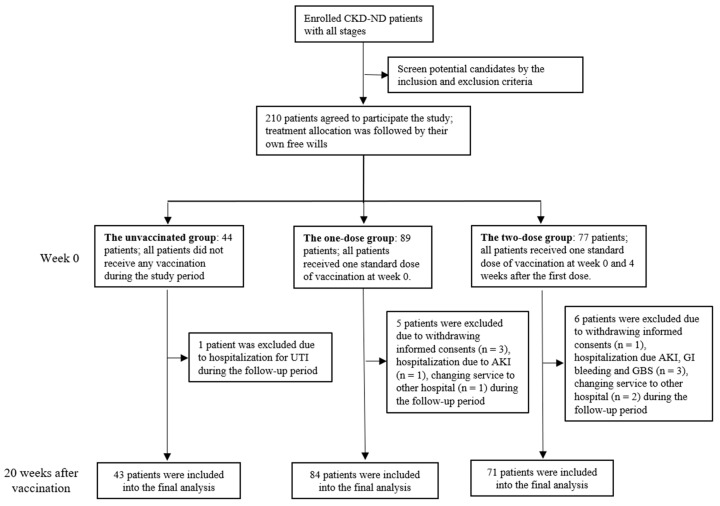
Methods: We conducted a single-center, non-randomized, open-label, controlled trial among patients with all stages of CKD-ND. Subjects were classified as unvaccinated, one-dose, and two-dose groups (4 weeks apart) after enrollment. Serial changes in immunological parameters (0, 4, 8, and 20 weeks after enrollment), including seroprotection, geometric mean titer (GMT), GMT fold-increase, seroconversion, and seroresponse, were applied to evaluate vaccine efficacy.
Results: There were 43, 84, and 71 patients in the unvaccinated, one-dose, and two-dose vaccination groups, respectively. At 4-8 weeks after vaccination, seroprotection rates in the one- and two-dose group for H1N1, H3N2, and B ranged from 82.6-95.8%, 97.4-100%, and 73.9-100%, respectively. The concomitant seroconversion and GMT fold-increases nearly met the suggested criteria for vaccine efficacy for the elderly population. Although the seroprotection rates for all of the groups were adequate, the seroconversion and GMT fold-increase at 20 weeks after vaccination did not meet the criteria for vaccine efficacy. The two-dose regimen had a higher probability of achieving seroprotection for B strains (Odds ratio: 3.5, 95% confidence interval (1.30-9.40)). No significant differences in vaccine efficacy were found between early (stage 1-3) and late (stage 4-5) stage CKD.
Conclusions: The standard one-dose vaccination can elicit sufficient protective antibodies. The two-dose regimen induced a better immune response when the baseline serum antibody titer was low. Monitoring change in antibody titers for a longer duration is warranted to further determine the current vaccine strategy in CKD-ND population.
Keywords: booster dosage; immune response; influenza virus; non-dialysis-dependent chronic kidney disease; vaccine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- World Health Organization Global Influenza Surveillance Network . Manual for the Laboratory Diagnosis and Virological Surveillance of Influenza. WHO; Geneva, Switzerland: 2011.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
