

Brain Metastases from Colorectal Cancer: A Systematic Review of the Literature and Meta-Analysis to Establish a Guideline for Daily Treatment
- PMID: 33669974
- PMCID: PMC7924831
- DOI: 10.3390/cancers13040900
Brain Metastases from Colorectal Cancer: A Systematic Review of the Literature and Meta-Analysis to Establish a Guideline for Daily Treatment
Abstract
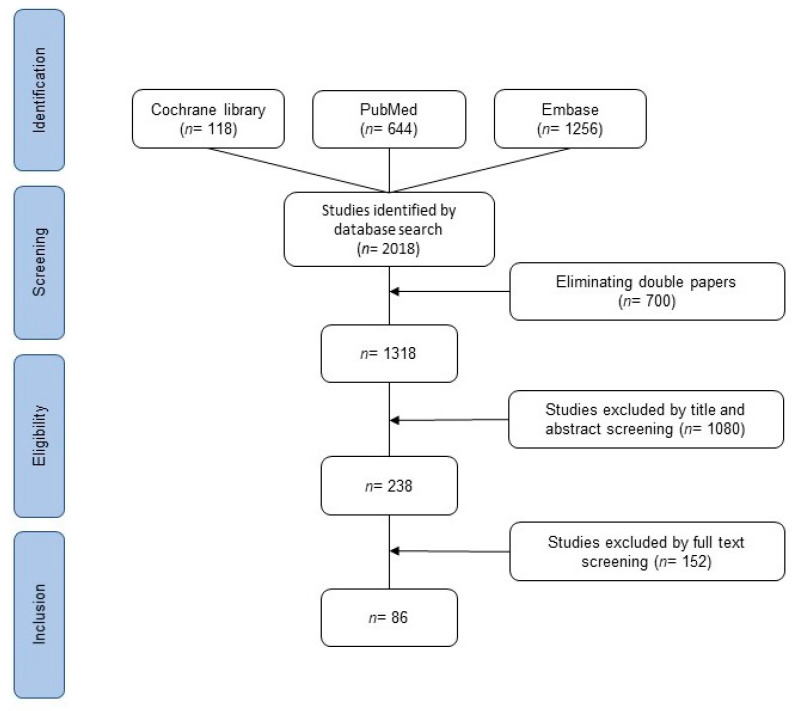
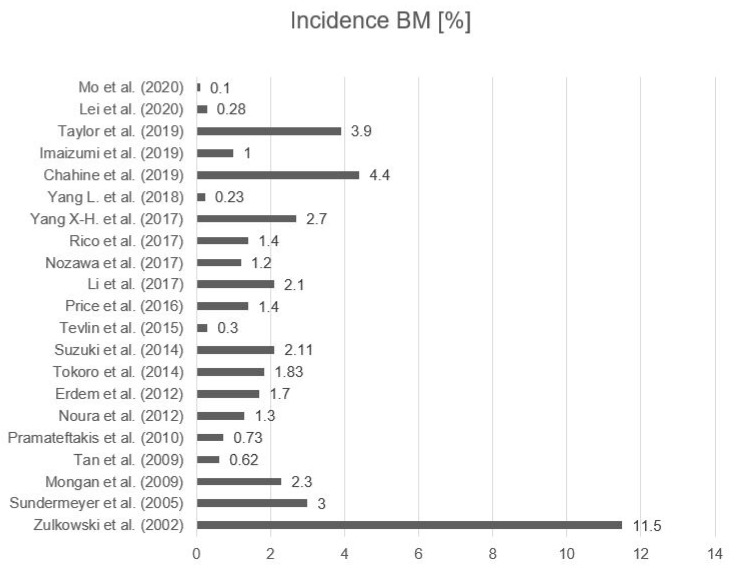
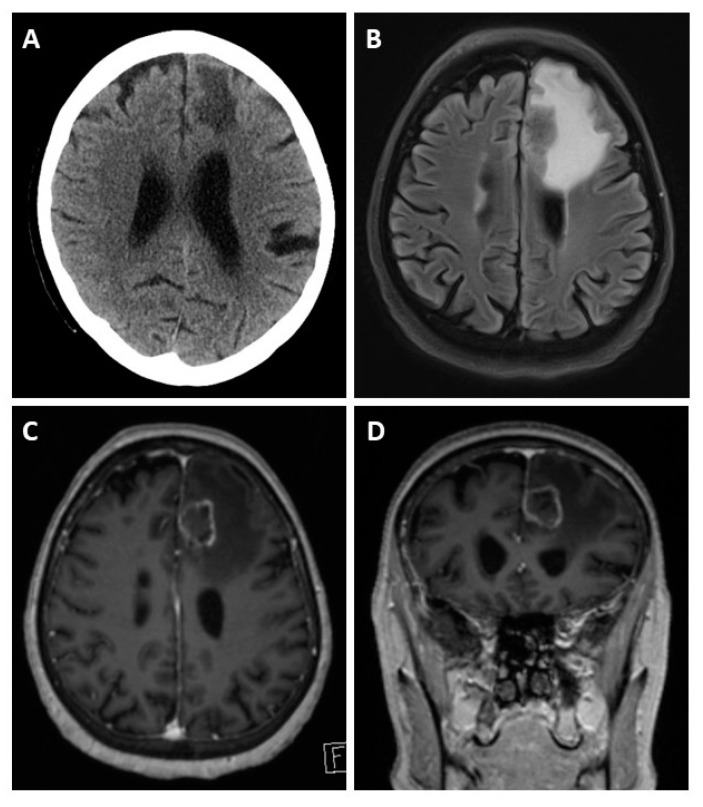
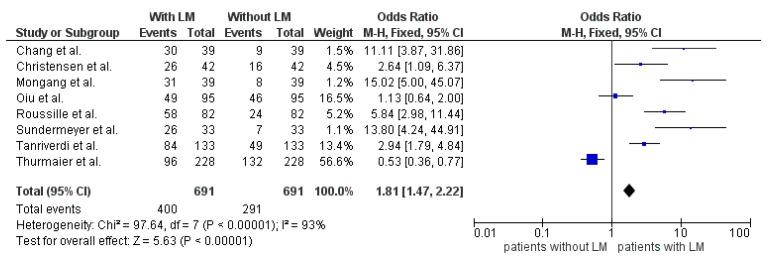
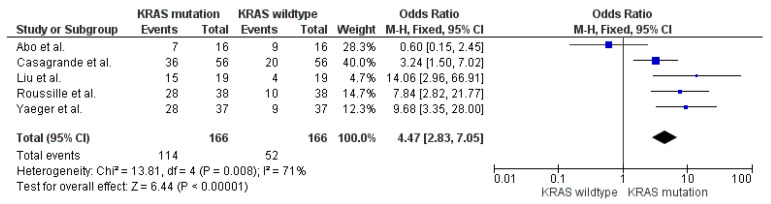
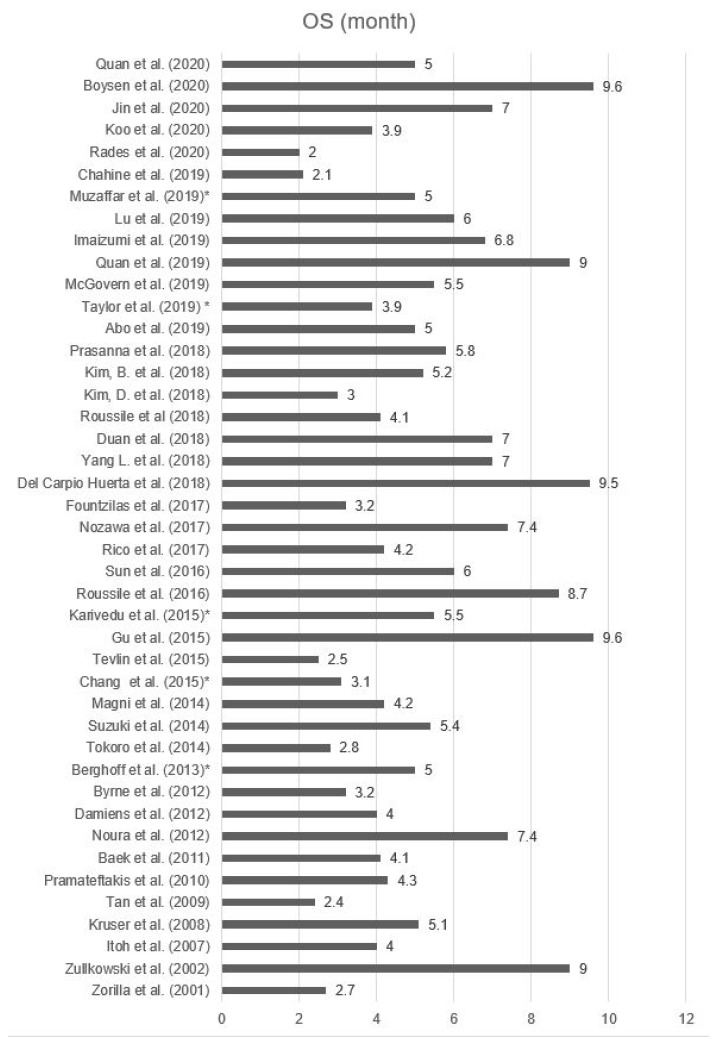
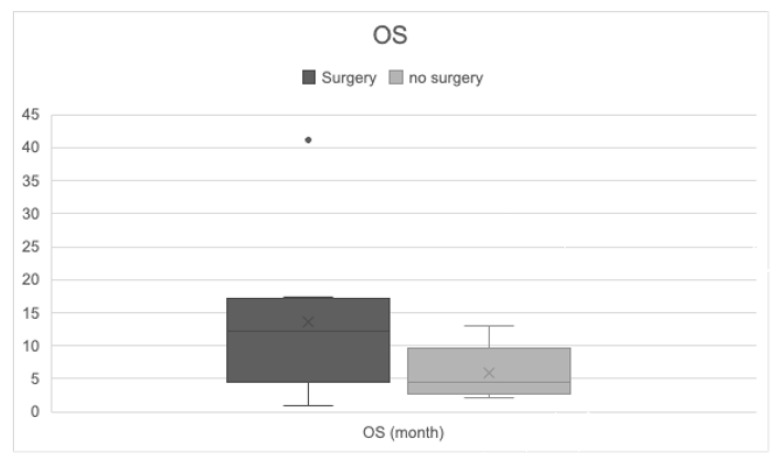
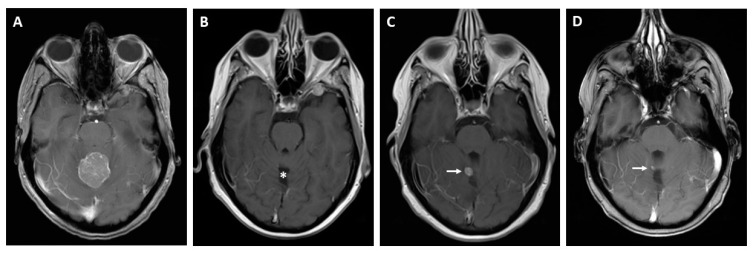
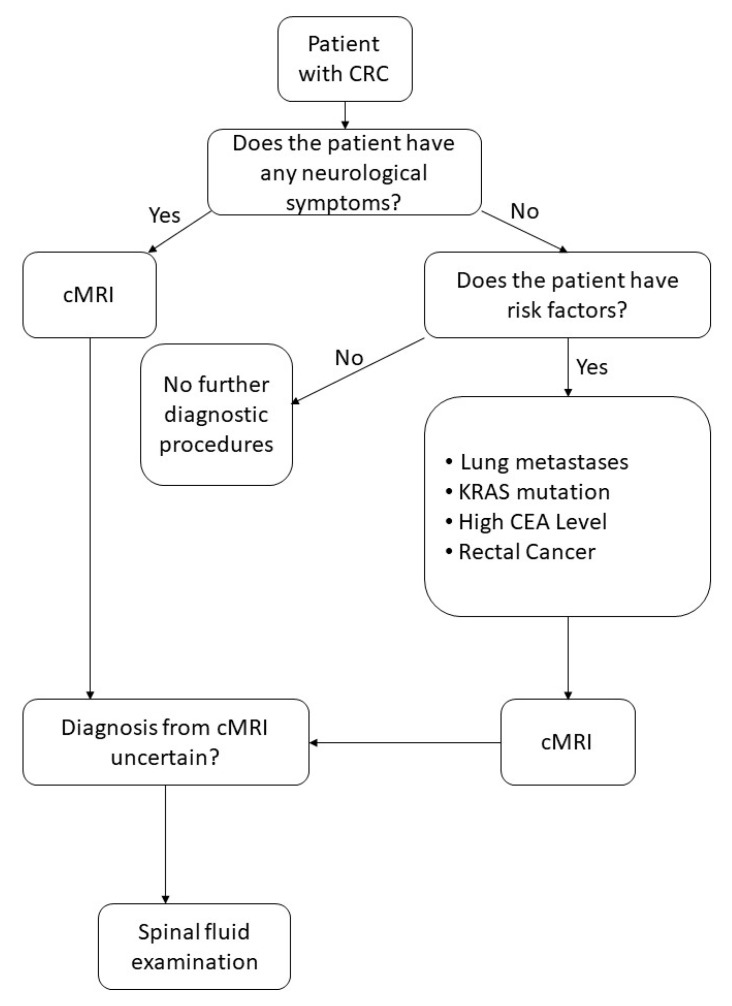
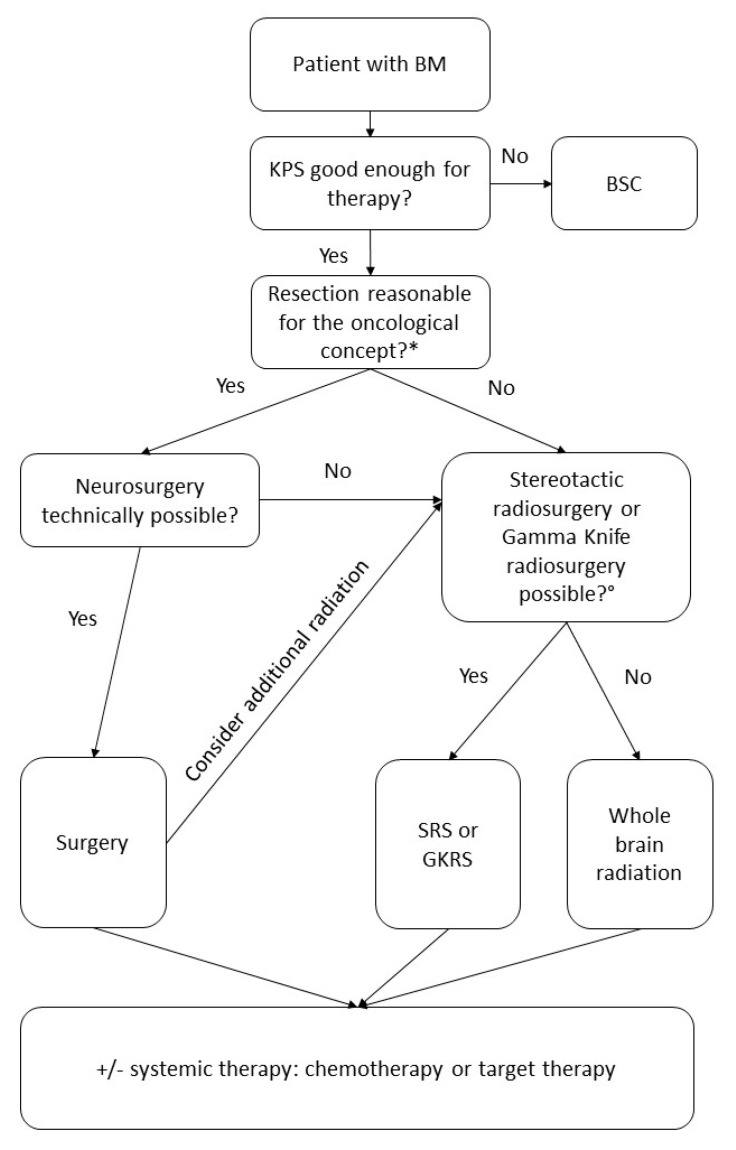
Colorectal cancer (CRC) is the third most common malignancy worldwide. Most patients with metastatic CRC develop liver or lung metastases, while a minority suffer from brain metastases. There is little information available regarding the presentation, treatment, and overall survival of brain metastases (BM) from CRC. This systematic review and meta-analysis includes data collected from three major databases (PubMed, Cochrane, and Embase) based on the key words "brain", "metastas*", "tumor", "colorectal", "cancer", and "malignancy". In total, 1318 articles were identified in the search and 86 studies matched the inclusion criteria. The incidence of BM varied between 0.1% and 11.5%. Most patients developed metastases at other sites prior to developing BM. Lung metastases and KRAS mutations were described as risk factors for additional BM. Patients with BM suffered from various symptoms, but up to 96.8% of BM patients were asymptomatic at the time of BM diagnosis. Median survival time ranged from 2 to 9.6 months, and overall survival (OS) increased up to 41.1 months in patients on a multimodal therapy regimen. Several factors including age, blood levels of carcinoembryonic antigen (CEA), multiple metastases sites, number of brain lesions, and presence of the KRAS mutation were predictors of OS. For BM diagnosis, MRI was considered to be state of the art. Treatment consisted of a combination of surgery, radiation, or systemic treatment.
Keywords: BM; CRC; brain metastases; cerebral metastases; colorectal cancer; meta-analysis; systematic review.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization Cancer Today; Number of Incident Cases and Deaths Worldwide. [(accessed on 5 January 2021)]; Available online: https://gco.iarc.fr/today/online-analysis-multi-bars?v=2018&mode=cancer&....
-
- Robert Koch Institute . Cancer in Germany 2015/2016—Colon and Rectum. Robert Koch Institute; Berlin, Germany: 2016.
-
- World Health Organization Cancer Today; Fact Sheet Colorectal. [(accessed on 5 January 2021)]; Available online: https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact....
-
- World Health Organization Cancer Survival. [(accessed on 5 January 2021)]; Available online: https://gco.iarc.fr/survival/survmark/visualizations/viz8/?cancer=%22Col....
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
