

Use of Phil Embolic Agent for Bleeding in Non-Neurological Interventions
- PMID: 33670124
- PMCID: PMC7916888
- DOI: 10.3390/jcm10040701
Use of Phil Embolic Agent for Bleeding in Non-Neurological Interventions
Abstract
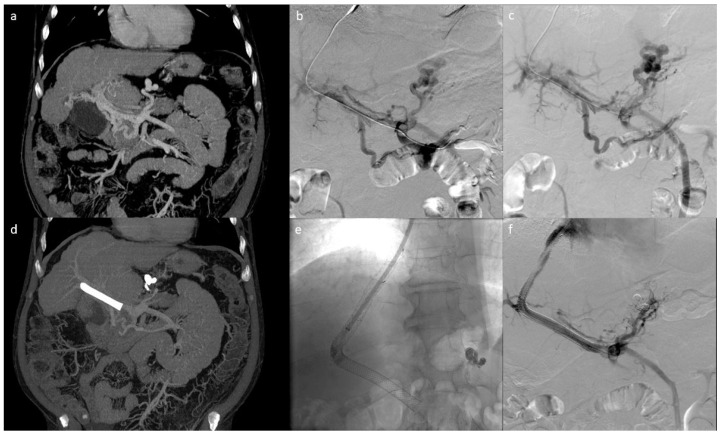
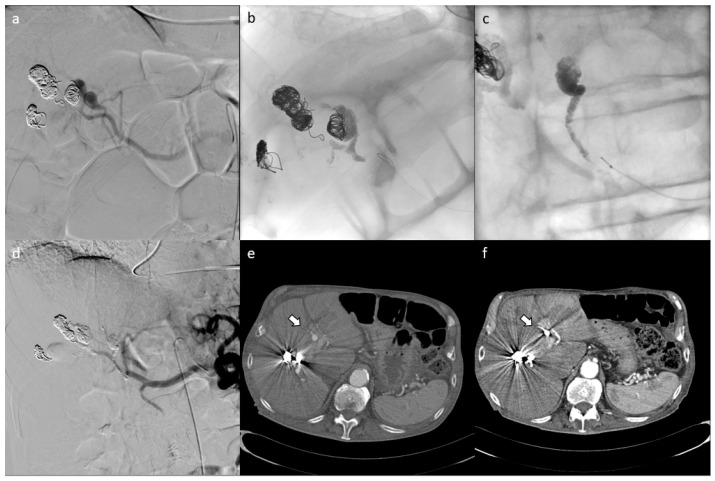
Objective: To evaluate the safety and efficacy of the Phil liquid embolic agent in non-neurological embolization procedures. M&M: Thirty-five patients with a mean age of 62.5 years underwent percutaneous embolization using Phil for the treatment of visceral arterial bleedings in 20/35 patients (including three gluteal, one bladder, two superior mesenteric, three epigastric, one deep femoral, five internal iliac, four intercostal, and one lingual arteries), splanchnic pseudoaneurysms in 11/35 patients (including three hepatic, five splenic, and three renal arteries), pancreatic bleeding metastasis in 1/35 patient, and gastric bleeding varices in 3/35 patients. Phil is composed of a non-adhesive copolymer dissolved in DMSO (Anhydrous Dimethyl Sulfoxide) with different viscosity. Procedures were performed slowly under continuous fluoroscopic guidance to avoid embolization of non-target vessels.
Results: Clinical success was obtained with a single intervention in 34 cases (97.15%), while a repeated procedure was required in one case (2.85%). No technical complications nor non-target embolization occurred. A case of post-embolic syndrome was noted (2.85%) in one patient. DMSO administration-related pain was successfully controlled by medical therapy.
Conclusion: Phil can be considered a safe and effective embolic agent for the treatment of non-neurologic bleeding.
Keywords: bleeding; liquid embolic agent; non-neurologic intervention; transcatheter embolization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Angle J.F., Siddiqi N.H., Wallace M.J., Kundu S., Stokes L., Wojak J.C., Cardella J.F. Quality improvement guidelines for percutaneous transcatheter embolization: Society of interventional radiology standards of practice committee. J. Vasc. Interv. Radiol. 2010;21:1479–1486. doi: 10.1016/j.jvir.2010.06.014. - DOI - PubMed
-
- Chakraverty S., Flood K., Kessel D., McPherson S., Nicholson T., Ray C.E., Jr., Robertson I., van Delden O.M. CIRSE guidelines: Quality improvement guidelines for endovascular treatment of traumatic hemorrhage. Cardiovasc. Interv. Radiol. 2012;35:472–482. doi: 10.1007/s00270-012-0339-7. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
