

Compound Sarcopenia in Hospitalized Patients with Cirrhosis Worsens Outcomes with Increasing Age
- PMID: 33670535
- PMCID: PMC7923160
- DOI: 10.3390/nu13020659
Compound Sarcopenia in Hospitalized Patients with Cirrhosis Worsens Outcomes with Increasing Age
Abstract
Background: There are limited data on outcomes of older patients with chronic diseases. Skeletal muscle loss of aging (primary sarcopenia) has been extensively studied but the impact of secondary sarcopenia of chronic disease is not as well evaluated. Older patients with chronic diseases have both primary and secondary sarcopenia that we term compound sarcopenia. We evaluated the clinical impact of compound sarcopenia in hospitalized patients with cirrhosis given the increasing number of patients and high prevalence of sarcopenia in these patients.
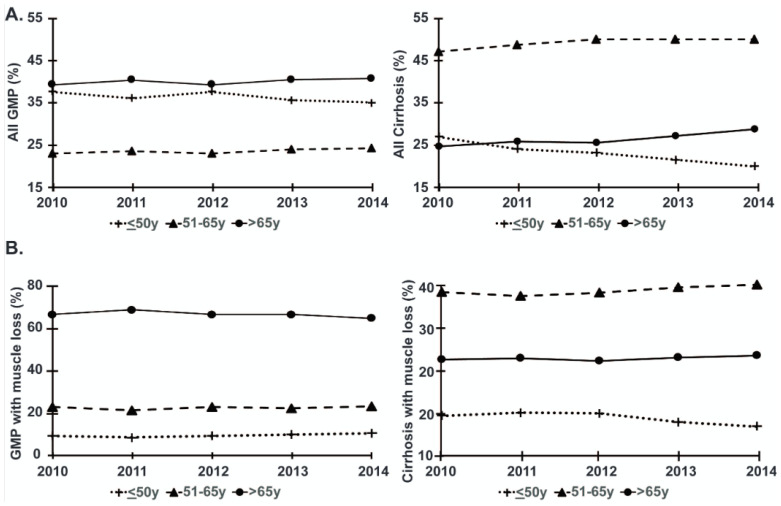
Design: The Nationwide Inpatients Sample (NIS) database (years 2010-2014) was analyzed to study older patients with cirrhosis. Since there is no universal hospital diagnosis code for "muscle loss", we used a comprehensive array of codes for "muscle loss phenotype" in the international classification of diseases-9 (ICD-9). A randomly selected 2% sample of hospitalized general medical population (GMP) and inpatients with cirrhosis were stratified into 3 age groups based on age-related changes in muscle mass. In-hospital mortality, length of stay (LoS), cost of hospitalization (CoH), comorbidities and discharge disposition were analyzed.
Results: Of 517,605 hospitalizations for GMP and 106,835 hospitalizations for treatment of cirrhosis or a cirrhosis-related complication, 207,266 (40.4%) GMP and 29,018 (27.7%) patients with cirrhosis were >65 years old, respectively. Muscle loss phenotype in both GMP and inpatients with cirrhosis 51-65 years old and >65 years old was significantly (p < 0.001 for all) associated with higher mortality, LoS, and CoH compared to those ≤50 years old. Patients >65 years old with cirrhosis and muscle loss phenotype had higher mortality (adjusted OR: 1.06, 95% CI [1.04, 1.08] and CoH (adjusted odds ratio (OR): 1.10, 95% confidence interval (CI) [1.04, 1.08])) when compared to >65 years old GMP with muscle loss phenotype. Muscle loss in younger patients with cirrhosis (≤50 years old) was associated with worse outcomes compared to GMP >65 years old. Non-home discharges (nursing, skilled, long-term care) were more frequent with increasing age to a greater extent in patients with cirrhosis with muscle loss phenotype for each age stratum.
Conclusion: Muscle loss is more frequent in older patients with cirrhosis than younger patients with cirrhosis and older GMP. Younger patients with cirrhosis had clinical outcomes similar to those of older GMP, suggesting an accelerated senescence in cirrhosis. Compound sarcopenia in older patients with cirrhosis is associated with higher inpatient mortality, increased LoS, and CoH compared to GMP with sarcopenia.
Keywords: aging; cirrhosis; clinical outcomes; cost of stay; inpatient mortality; sarcopenia.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Ortman J.M., Velkoff V.A., Hogan H. An Aging Nation: The Older Population in the United States. U.S. Census Bureau; Washington, DC, USA: 2014. Current Population Reports P25-1140.
-
- Kim D., Li A.A., Perumpail B.J., Gadiparthi C., Kim W., Cholankeril G., Glenn J.S., Harrison S.A., Younossi Z.M., Ahmed A. Changing Trends in Etiology-Based and Ethnicity-Based Annual Mortality Rates of Cirrhosis and Hepatocellular Carcinoma in the United States. Hepatology. 2019;69:1064–1074. doi: 10.1002/hep.30161. - DOI - PMC - PubMed
-
- van Vugt J.L.A., Buettner S., Alferink L.J.M., Bossche N., de Bruin R.W.F., Darwish Murad S., Polak W.G., Metselaar H.J., IJzermans J.N.M. Low skeletal muscle mass is associated with increased hospital costs in patients with cirrhosis listed for liver transplantation-a retrospective study. Transpl. Int. 2018;31:165–174. doi: 10.1111/tri.13048. - DOI - PubMed
MeSH terms
Grants and funding
- K08 AA028794/AA/NIAAA NIH HHS/United States
- K12 HL141952/HL/NHLBI NIH HHS/United States
- R21 AR 071046; RO1 GM119174; RO1 DK113196; P50 AA024333; RO1 AA021890; 3U01AA026976 - 03S1; UO1 AA 026976; R56HL141744;UO1 DK061732; 5U01DK062470-17S2 (SD); K12 HL141952 and the American College of Gastroenterology Clinical Research Award (NW)./NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
