

Negligible Correlation between Radiographic Measurements and Clinical Outcomes in Patients Following Primary Reverse Total Shoulder Arthroplasty
- PMID: 33671318
- PMCID: PMC7923193
- DOI: 10.3390/jcm10040809
Negligible Correlation between Radiographic Measurements and Clinical Outcomes in Patients Following Primary Reverse Total Shoulder Arthroplasty
Abstract
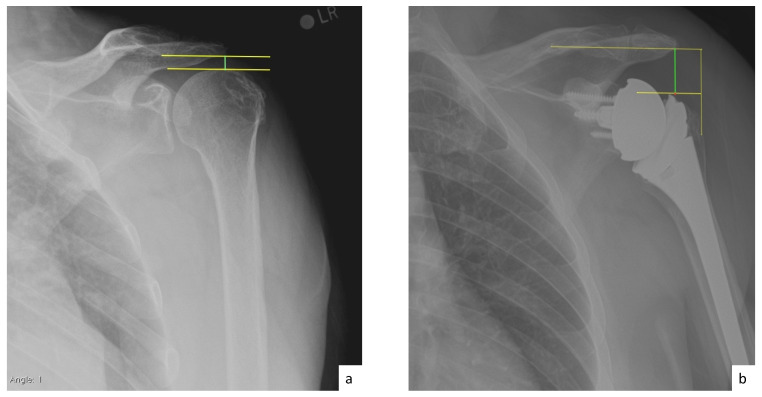
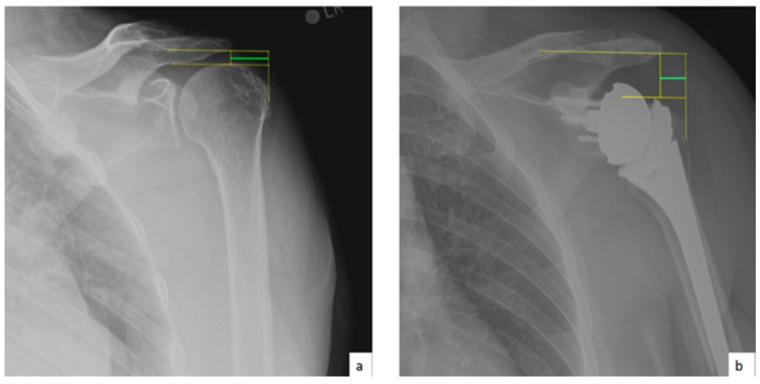
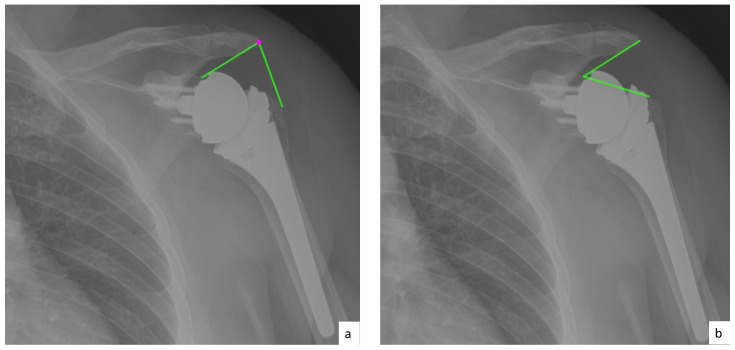
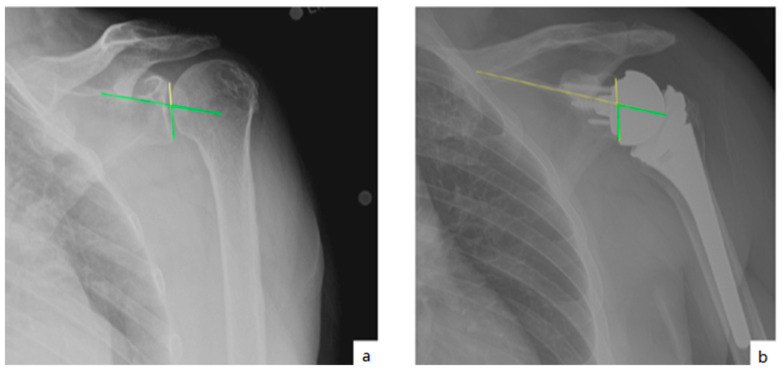
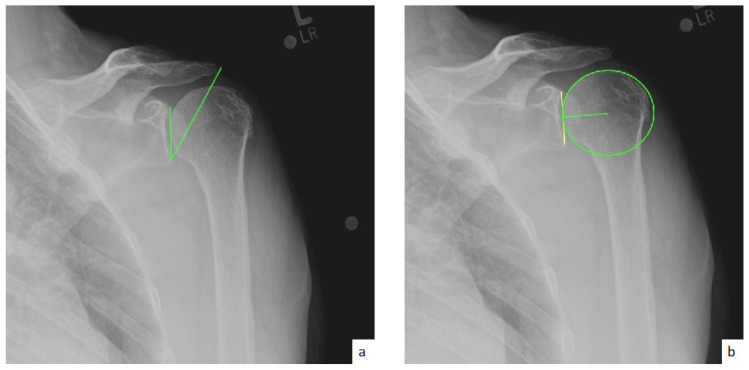
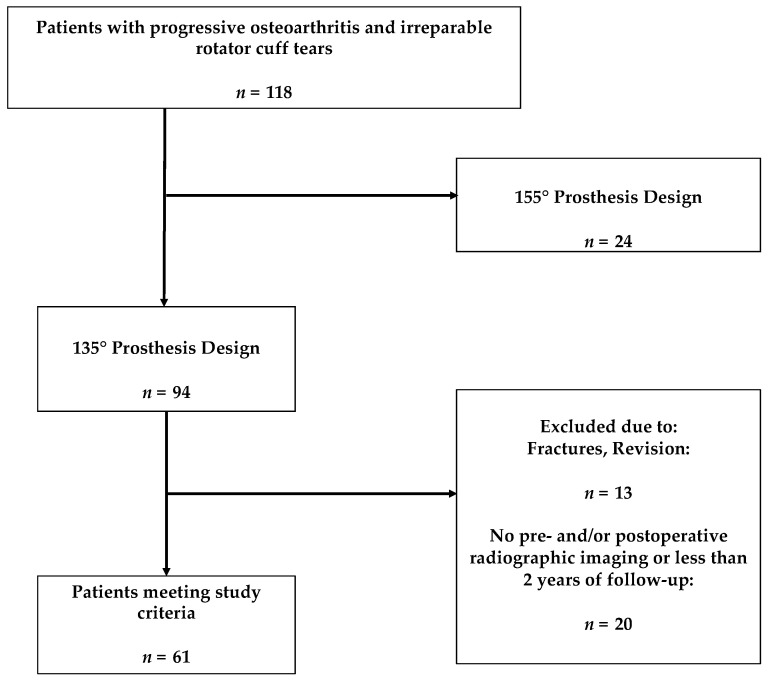
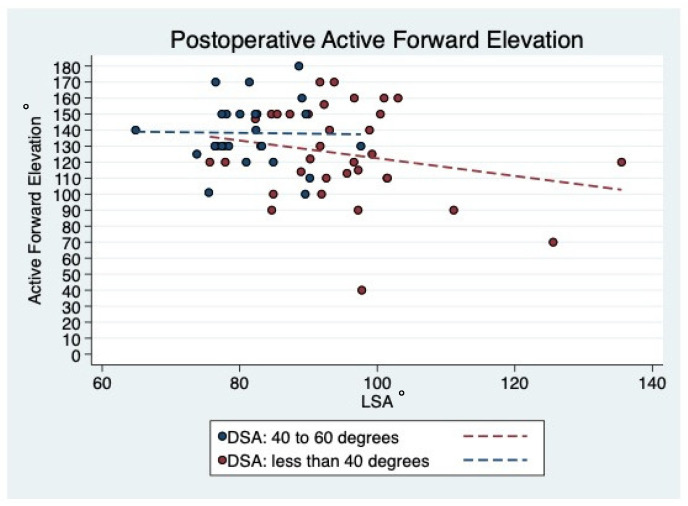
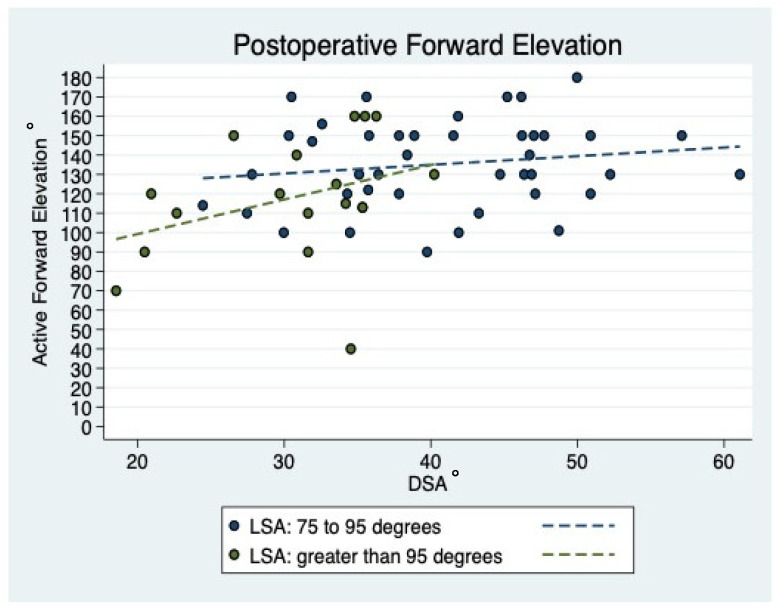
Previous attempts to measure lateralization, distalization or inclination after reverse total shoulder arthroplasty (rTSA) and to correlate them with clinical outcomes have been made in the past years. However, this is considered to be too demanding and challenging for daily clinical practice. Additionally, the reported findings were obtained from heterogeneous rTSA cohorts using 145° and 155° designs and are limited in external validity. The purpose of this study was to investigate the prognostic preoperative and postoperative radiographic factors affecting clinical outcomes in patients following rTSA using a 135° prosthesis design. In a multi-center design, patients undergoing primary rTSA using a 135° design were included. Radiographic analysis included center of rotation (COR), acromiohumeral distance (AHD), lateral humeral offset (LHO), distalization shoulder angle (DSA), lateralization shoulder angle (LSA), critical shoulder angle (CSA), and glenoid and baseplate inclination. Radiographic measurements were correlated to clinical and functional outcomes, including the American Shoulder and Elbow Surgeons (ASES), Simple Shoulder Test (STT), Single Assessment Numeric Evaluation (SANE), and Visual Analogue Scale (VAS) score, active forward elevation (AFE), external rotation (AER), and abduction (AABD), at a minimum 2-year follow-up. There was a significant correlation between both DSA (r = 0.299; p = 0.020) and LSA (r = -0.276; p = 0.033) and the degree of AFE at final follow-up. However, no correlation between DSA (r = 0.133; p = 0.317) and LSA (r = -0.096; p = 0.471) and AER was observed. Postoperative AHD demonstrated a significant correlation with final AFE (r = 0.398; p = 0.002) and SST (r = 0.293; p = 0.025). Further, postoperative LHO showed a significant correlation with ASES (r = -0.281; p = 0.030) and LSA showed a significant correlation with ASES (r = -0.327; p = 0.011), SANE (r = -0.308, p = 0.012), SST (r = -0.410; p = 0.001), and VAS (r = 0.272; p = 0.034) at terminal follow-up. All other correlations were found to be non-significant (p > 0.05, respectively). Negligible correlations between pre- and postoperative radiographic measurements and clinical outcomes following primary rTSA using a 135° prosthesis design were demonstrated; however, these observations are of limited predictive value for outcomes following rTSA. Subsequently, there remains a debate regarding the ideal placement of the components during rTSA to most sufficiently restore active ROM while minimizing complications such as component loosening and scapular notching. Additionally, as the data from this study show, there is still a considerable lack of data in assessing radiographic prosthesis positioning in correlation to clinical outcomes. As such, the importance of radiographic measurements and their correlation with clinical and functional outcomes following rTSA may be limited.
Keywords: DSA; LSA; distalization; lateralization; radiographic analysis; reverse total shoulder arthroplasty.
Conflict of interest statement
Authors B.D.P., M.D., M.L.M. and B.J.B., C.A.R. declare that they have no conflict of interest. A.D.M. reports research grants from Arthrex Inc., is a consultant for Arthrex Inc. and receives royalties from Arthrex Inc. D.P.J. is a consultant for Arthrex Inc. and receives royalties from Arthrex Inc. L.E. is a consultant for Arthrex Inc. and receives royalties from Arthrex Inc. C.M.P. receives personal fees from Arthroscopy Association of North America (AANA). Gobezie R is a consultant for Arthrex Inc. and receives royalties from Arthrex Inc. R.A.R. receives material or orther financial support from AANA; is a board or committee member of Amercian Shoulder and Elbow Surgeons; Receives financial and material support from Arthrex Inc. ansd receives royalties from Arthrex Inc; receives other financial or material support from Mayor League Baseball; is an Editorial or governing board for Orthopedics and a board or committee member for Orthopedics Today; receives research support from Paragen Technologies and holds stock or stock options for Paragen Technologies; Is an editorial or governing board for SAGE; receives royalties and material support by Saunders/Mosby-Elsevier; receives royalties or material support for SLACK incorporated and is a editorial or governing board for SLACK incorporated; is an editorial or governing board for Wolters Kluwer Health. K Beitzel is a consultant for Arthrex Inc. and receives royalties from Arthrex Inc.
Figures
References
-
- Routman H.D., Flurin P.H., Wright T.W., Zuckerman J.D., Hamilton M.A., Roche C.P. Reverse Shoulder Arthroplasty Prosthesis Design Classification System. Bull. NYU Hosp. Jt. Dis. 2015;73:S5–S14. - PubMed
-
- Grammont P. Etude et réalisation d’une nouvelle prothèse d’épaule. Rheumatologie. 1987;39:27–38.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
