

Pyonephrosis Ultrasound and Computed Tomography Features: A Pictorial Review
- PMID: 33671431
- PMCID: PMC7921924
- DOI: 10.3390/diagnostics11020331
Pyonephrosis Ultrasound and Computed Tomography Features: A Pictorial Review
Abstract
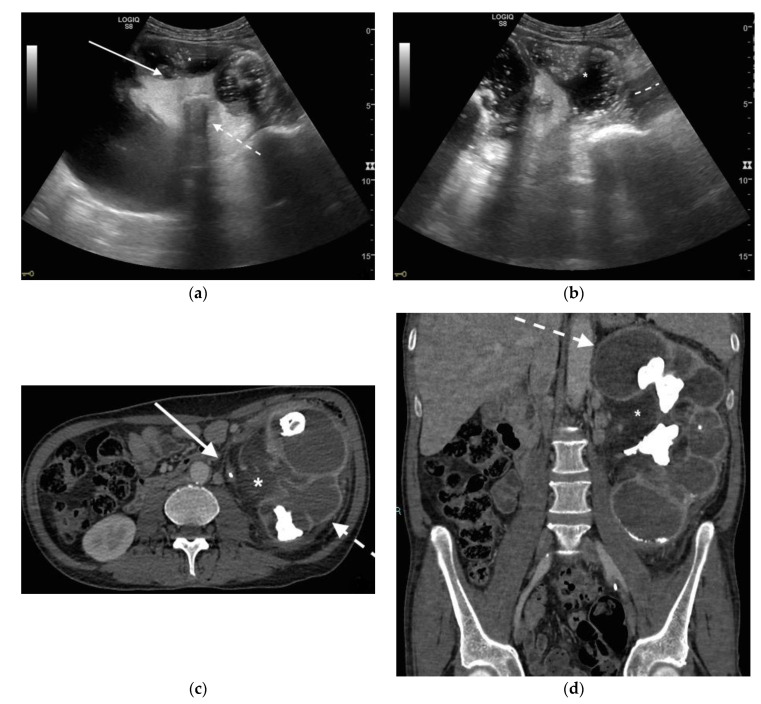
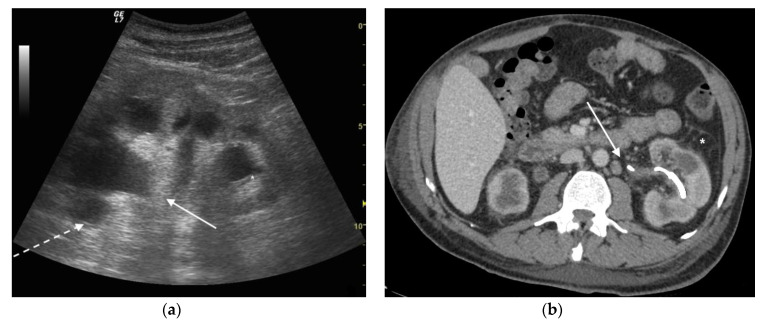
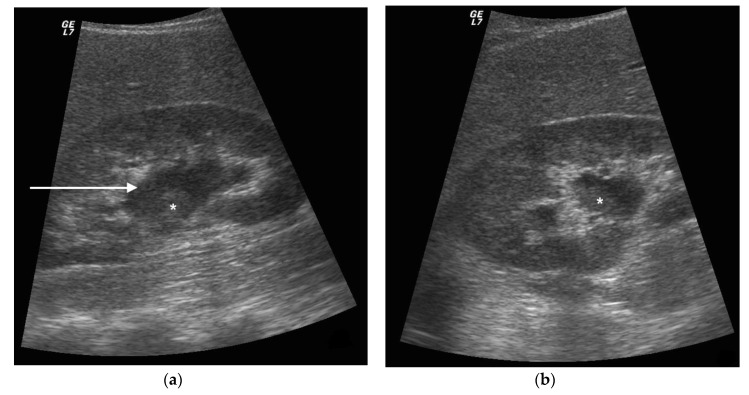
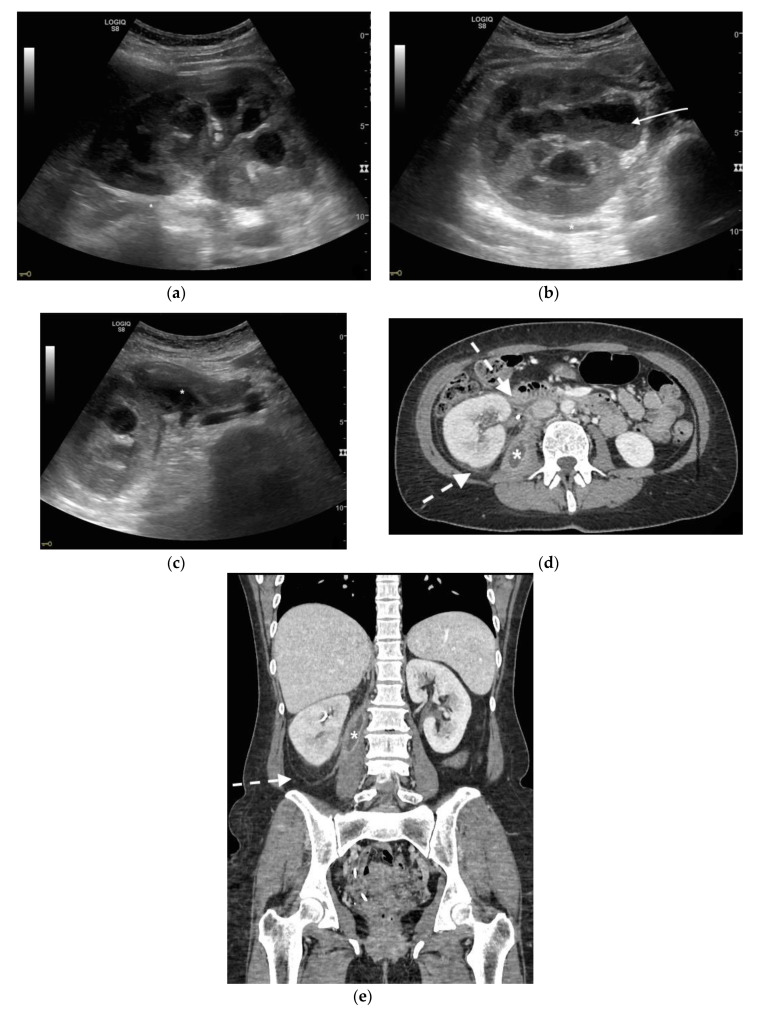
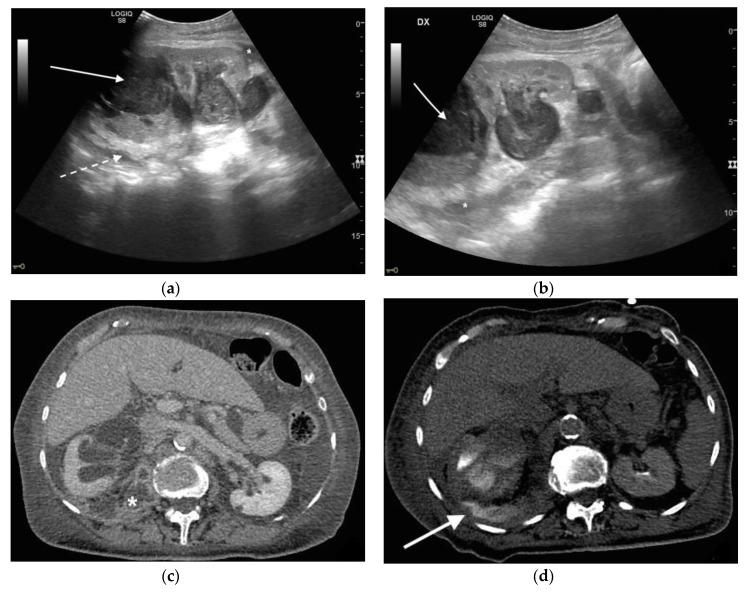
Urinary tract infections (UTIs) are the most frequent community-acquired and healthcare-associated bacterial infections. UTIs are heterogeneous and range from rather benign, uncomplicated infections to complicated UTIs (cUTIs), pyelonephritis and severe urosepsis, depending mostly on the host response. Ultrasound and computed tomography represent the imaging processes of choice in the diagnosis and staging of the pathology in emergency settings. The aim of this study is to describe the common ultrasound (US) and computed tomography (CT) features of pyonephrosis. US can make the diagnosis, demonstrating echogenic debris, fluid/fluid levels, and air in the collecting system. Although the diagnosis appears to be easily made with US, CT is necessary in non-diagnostic US examinations to confirm the diagnosis, to demonstrate the cause and moreover to stage the pathology, defining extrarenal complications. In emergency settings, US and CT are differently used in the diagnosis and staging of pyonephrosis.
Keywords: CT; US; pyonephrosis; sepsis; urinary tract infections.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
