

IMPELLA® or Extracorporeal Membrane Oxygenation for Left Ventricular Dominant Refractory Cardiogenic Shock
- PMID: 33672792
- PMCID: PMC7918655
- DOI: 10.3390/jcm10040759
IMPELLA® or Extracorporeal Membrane Oxygenation for Left Ventricular Dominant Refractory Cardiogenic Shock
Abstract
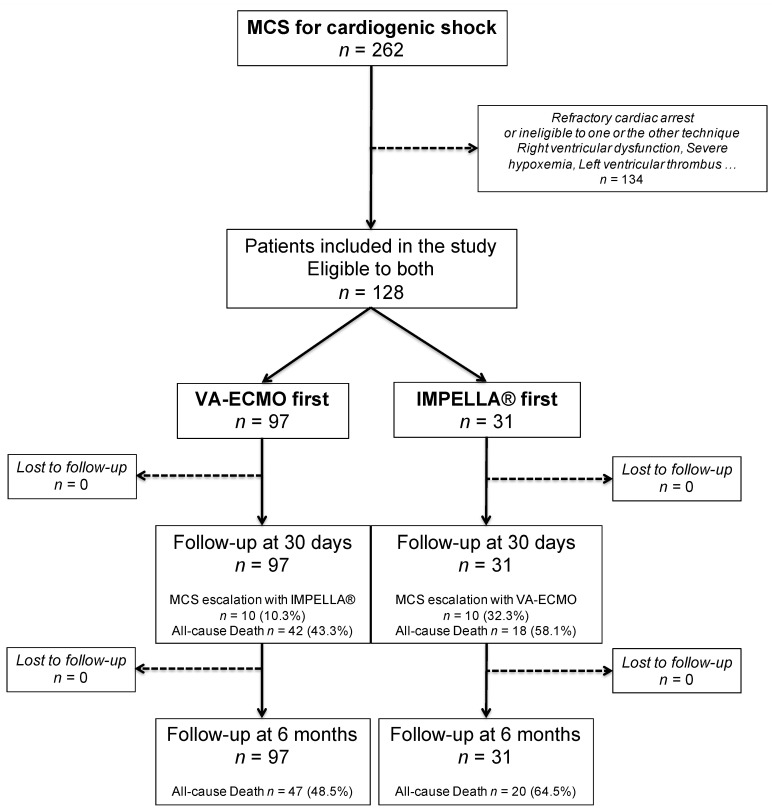
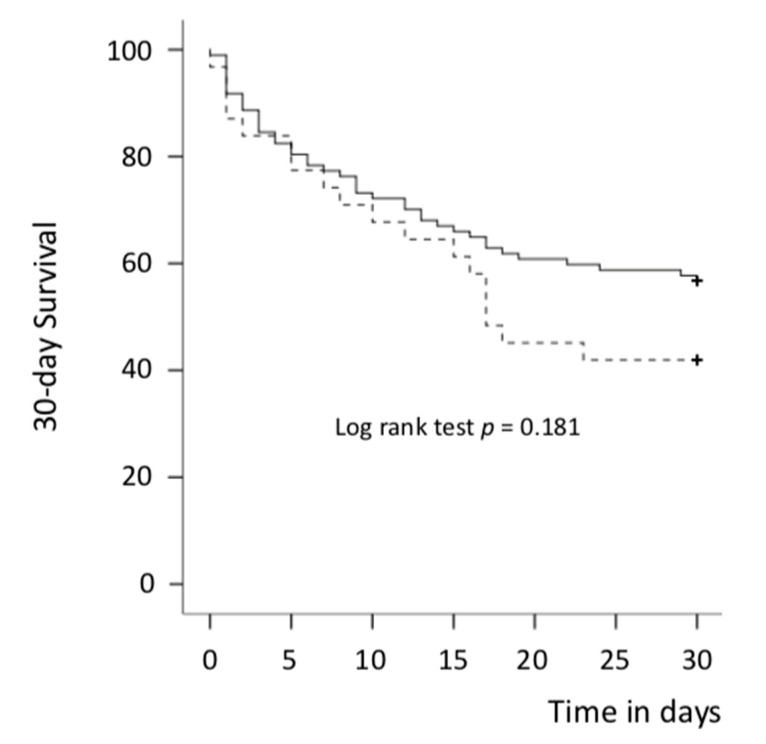
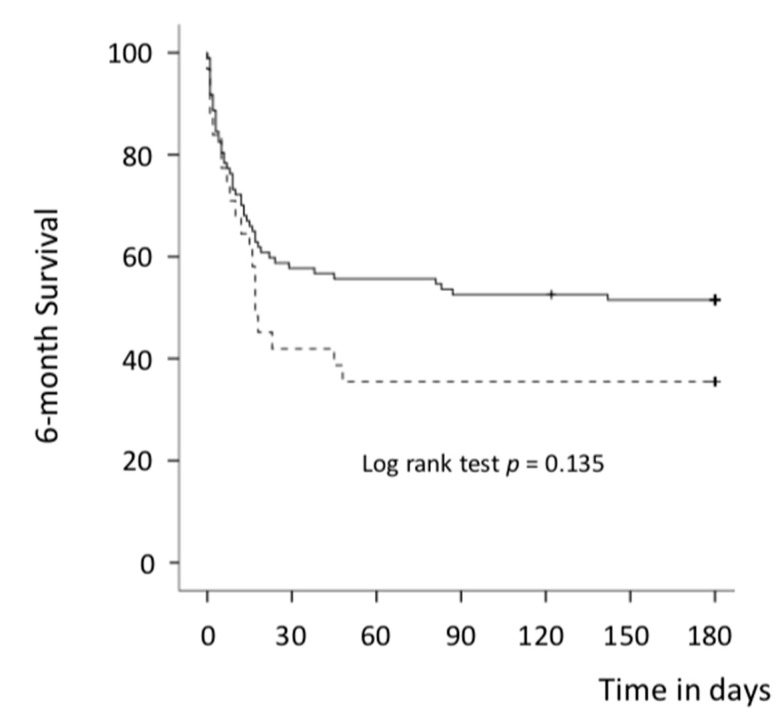
Mechanical circulatory support (MCS) devices are effective tools in managing refractory cardiogenic shock (CS). Data comparing veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and IMPELLA® are however scarce. We aimed to assess outcomes of patients implanted with these two devices and eligible to both systems. From 2004 to 2020, we retrospectively analyzed 128 patients who underwent VA-ECMO or IMPELLA® in our institution for refractory left ventricle (LV) dominant CS. All patients were eligible to both systems: 97 patients were first implanted with VA-ECMO and 31 with IMPELLA®. The primary endpoint was 30-day all-cause death. VA-ECMO patients were younger (52 vs. 59.4, p = 0.006) and had a higher lactate level at baseline than those in the IMPELLA® group (6.84 vs. 3.03 mmol/L, p < 0.001). Duration of MCS was similar between groups (9.4 days vs. 6 days in the VA-ECMO and IMPELLA® groups respectively, p = 0.077). In unadjusted analysis, no significant difference was observed between groups in 30-day mortality: 43.3% vs. 58.1% in the VA-ECMO and IMPELLA® groups, respectively (p = 0.152). After adjustment, VA-ECMO was associated with a significant reduction in 30-day mortality (HR = 0.25, p = 0.004). A higher rate of MCS escalation was observed in the IMPELLA® group: 32.3% vs. 10.3% (p = 0.003). In patients eligible to either VA-ECMO or IMPELLA® for LV dominant refractory CS, VA-ECMO was associated with improved survival rate and a lower need for escalation.
Keywords: IMPELLA®; cardiogenic shock; extracorporeal membrane oxygenation; mechanical circulatory support.
Conflict of interest statement
All authors have disclosed that they do not have any conflicts of interest in direct connection with this article.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
