

International Practice Variability in Treatment of Aneurysmal Subarachnoid Hemorrhage
- PMID: 33672807
- PMCID: PMC7917699
- DOI: 10.3390/jcm10040762
International Practice Variability in Treatment of Aneurysmal Subarachnoid Hemorrhage
Abstract
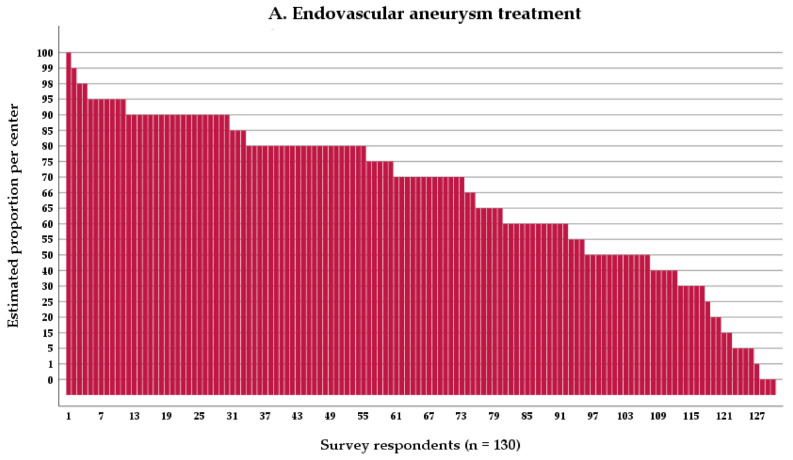
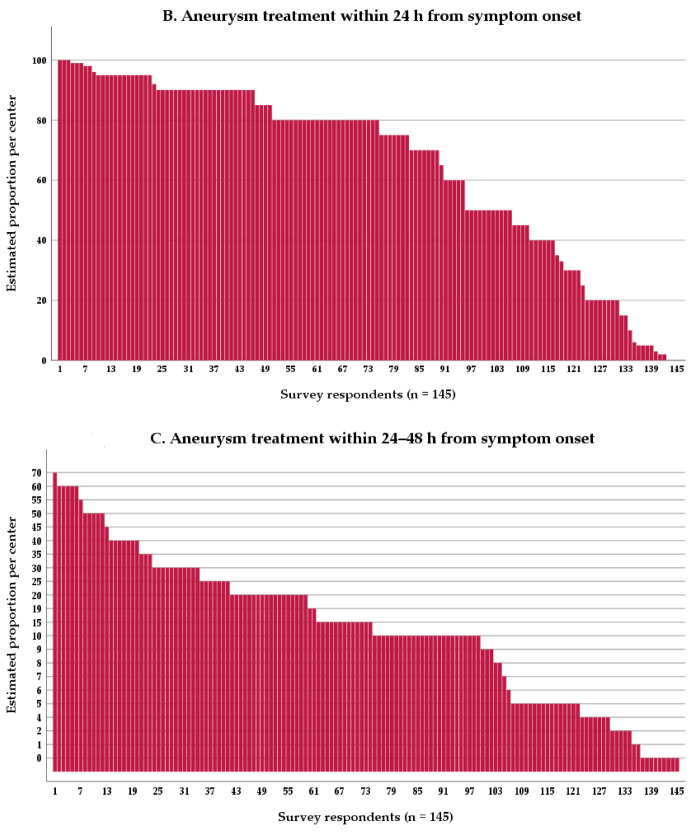
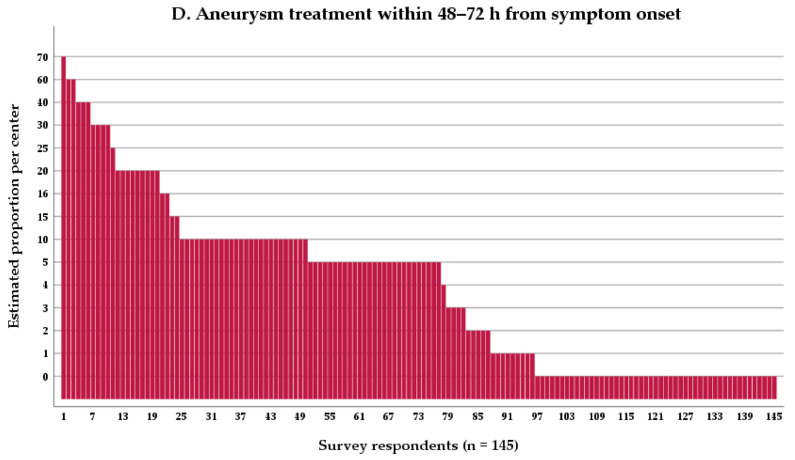
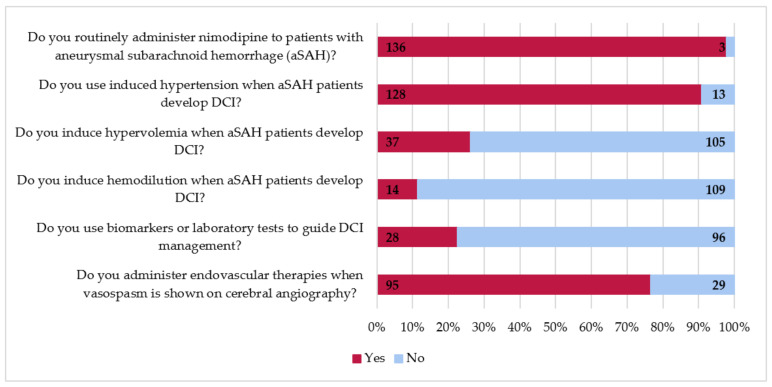
Prior research suggests substantial between-center differences in functional outcome following aneurysmal subarachnoid hemorrhage (aSAH). One hypothesis is that these differences are due to practice variability. To characterize practice variability, we sent a survey to 230 centers, of which 145 (63%) responded. Survey respondents indicated that an estimated 65% of ruptured aneurysms were treated endovascularly. Sixty-five percent of aneurysms were treated within 24 h of symptom onset, 18% within 24-48 h, and eight percent within 48-72 h. Centers in the United States (US) and Europe (EU) treat aneurysms more often endovascularly (72% and 70% vs. 51%, respectively, US vs. other p < 0.001, and EU vs. other p < 0.01) and more often within 24 h (77% and 64% vs. 46%, respectively, US vs. other p < 0.001, EU vs. other p < 0.01) compared to other centers. Most centers aim for euvolemia (96%) by administrating intravenous fluids to 0 (53%) or +500 mL/day (41%) net fluid balance. Induced hypertension is more often used in US centers (100%) than in EU (87%, p < 0.05) and other centers (81%, p < 0.05), and endovascular therapies for cerebral vasospasm are used more often in US centers than in other centers (91% and 60%, respectively, p < 0.05). We observed significant practice variability in aSAH treatment worldwide. Future comparative effectiveness research studies are needed to investigate how practice variation leads to differences in functional outcome.
Keywords: aneurysm treatment; delayed cerebral ischemia; fluid management; outcome; practice variation; subarachnoid hemorrhage; vasospasm.
Conflict of interest statement
Authors report no conflict of interest.
Figures

References
-
- Connolly E.S., Jr., Rabinstein A.A., Carhuapoma J.R., Derdeyn C.P., Dion J., Higashida R.T., Hoh B.L., Kirkness C.J., Naidech A.M., Ogilvy C.S., et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43:1711–1737. doi: 10.1161/STR.0b013e3182587839. - DOI - PubMed
-
- Etminan N., Chang H.S., Hackenberg K., de Rooij N.K., Vergouwen M.D.I., Rinkel G.J.E., Algra A. Worldwide Incidence of Aneurysmal Subarachnoid Hemorrhage According to Region, Time Period, Blood Pressure, and Smoking Prevalence in the Population: A Systematic Review and Meta-analysis. JAMA Neurol. 2019;76:588–597. doi: 10.1001/jamaneurol.2019.0006. - DOI - PMC - PubMed
-
- Go A.S., Mozaffarian D., Roger V.L., Benjamin E.J., Berry J.D., Blaha M.J., Dai S., Ford E.S., Fox C.S., Franco S., et al. Heart Disease and Stroke Statistics--2014 Update: A Report From the American Heart Association. Circulation. 2013;129:e28–e292. doi: 10.1161/01.cir.0000441139.02102.80. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
