

Role of the Macrophage Migration Inhibitory Factor in the Pathophysiology of Pre-Eclampsia
- PMID: 33673075
- PMCID: PMC7917653
- DOI: 10.3390/ijms22041823
Role of the Macrophage Migration Inhibitory Factor in the Pathophysiology of Pre-Eclampsia
Abstract
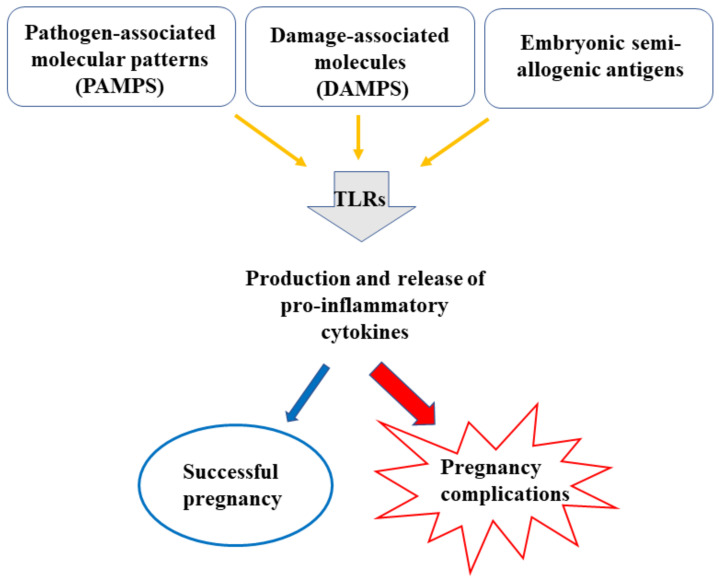
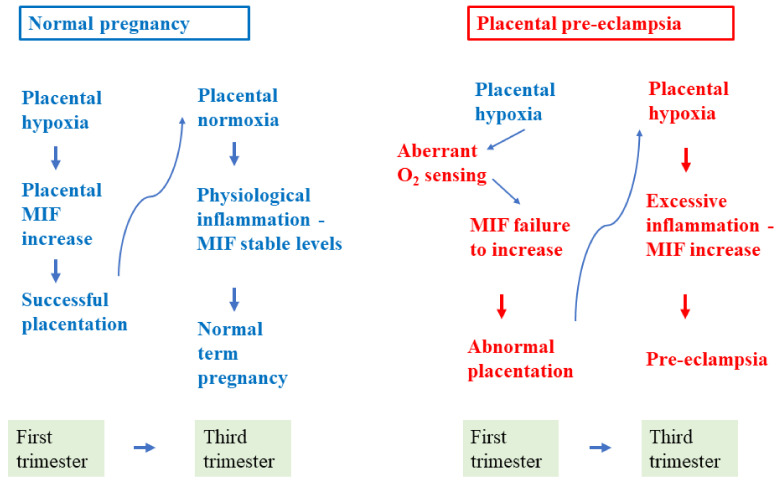
Proinflammatory cytokines are produced in pregnancy in response to the invading pathogens and/or nonmicrobial causes such as damage-associated molecules and embryonic semi-allogenic antigens. While inflammation is essential for a successful pregnancy, an excessive inflammatory response is implicated in several pathologies including pre-eclampsia (PE). This review focuses on the proinflammatory cytokine macrophage migration inhibitory factor (MIF), a critical regulator of the innate immune response and a major player of processes allowing normal placental development. PE is a severe pregnancy-related syndrome characterized by exaggerated inflammatory response and generalized endothelial damage. In some cases, usually of early onset, it originates from a maldevelopment of the placenta, and is associated with intrauterine growth restriction (IUGR) (placental PE). In other cases, usually of late onset, pre-pregnancy maternal diseases represent risk factors for the development of the disease (maternal PE). Available data suggest that low MIF production in early pregnancy could contribute to the abnormal placentation. The resulting placental hypoxia in later pregnancy could produce high release of MIF in maternal serum typical of placental PE. More studies are needed to understand the role of MIF, if any, in maternal PE.
Keywords: cytokines; human pregnancy; inflammatory response; placenta.
Conflict of interest statement
The authors declare no conflict of interest
Figures
References
-
- Brown M.A., Magee L.A., Kenny L.C., Karumanchi S.A., McCarthy F.P., Saito S., Hall D.R., Warren C.E., Adoyi G., Ishaku S., et al. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72:24–43. doi: 10.1161/HYPERTENSIONAHA.117.10803. - DOI - PubMed
-
- ACOG Practice Bulletin Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. Obs. Gynecol. 2002;99:159–167. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
