

Radio-Iodide Treatment: From Molecular Aspects to the Clinical View
- PMID: 33673669
- PMCID: PMC7957486
- DOI: 10.3390/cancers13050995
Radio-Iodide Treatment: From Molecular Aspects to the Clinical View
Abstract
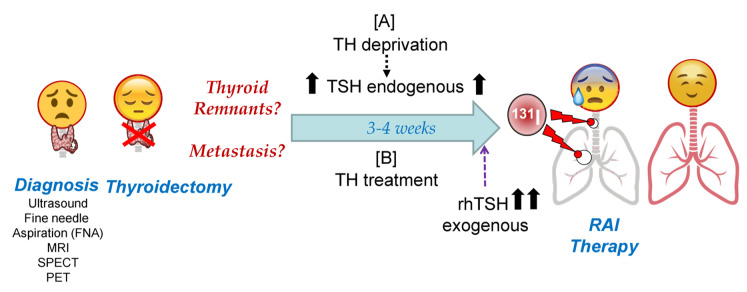
Thyroid radio-iodide therapy (RAI) is one of the oldest known and used targeted therapies. In thyroid cancer, it has been used for more than eight decades and is still being used to improve thyroid tumor treatment to eliminate remnants after thyroid surgery, and tumor metastases. Knowledge at the molecular level of the genes/proteins involved in the process has led to improvements in therapy, both from the point of view of when, how much, and how to use the therapy according to tumor type. The effectiveness of this therapy has spread into other types of targeted therapies, and this has made sodium/iodide symporter (NIS) one of the favorite theragnostic tools. Here we focus on describing the molecular mechanisms involved in radio-iodide therapy and how the alteration of these mechanisms in thyroid tumor progression affects the diagnosis and results of therapy in the clinic. We analyze basic questions when facing treatment, such as: (1) how the incorporation of radioiodine in normal, tumor, and metastatic thyroid cells occurs and how it is regulated; (2) the pros and cons of thyroid hormonal deprivation vs. recombinant human Thyroid Stimulating Hormone (rhTSH) in radioiodine residence time, treatment efficacy, thyroglobulin levels and organification, and its influence on diagnostic imaging tests and metastasis treatment; and (3) the effect of stunning and the possible causes. We discuss the possible incorporation of massive sequencing data into clinical practice, and we conclude with a socioeconomical and clinical vision of the above aspects.
Keywords: adjuvant therapy; differentiated thyroid cancer; radio-iodide treatment; radio-iodine-refractory thyroid cancer; recombinant human TSH; sodium/iodide symporter (NIS); stunning; theragnostic; thyroid cancer; thyroid hormonal deprivation.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures


Similar articles
-
Radioiodine-Refractory Thyroid Cancer: Molecular Basis of Redifferentiation Therapies, Management, and Novel Therapies.Cancers (Basel). 2019 Sep 17;11(9):1382. doi: 10.3390/cancers11091382. Cancers (Basel). 2019. PMID: 31533238 Free PMC article. Review.
-
Down-regulation of the sodium/iodide symporter explains 131I-induced thyroid stunning.Cancer Res. 2007 Aug 1;67(15):7512-7. doi: 10.1158/0008-5472.CAN-07-0823. Cancer Res. 2007. PMID: 17671222
-
Lithium as adjuvant to radioiodine therapy in differentiated thyroid carcinoma: clinical and in vitro studies.Clin Endocrinol (Oxf). 2006 Jun;64(6):617-24. doi: 10.1111/j.1365-2265.2006.02515.x. Clin Endocrinol (Oxf). 2006. PMID: 16712662
-
Enhancement of sodium/iodide symporter expression in thyroid and breast cancer.Endocr Relat Cancer. 2006 Sep;13(3):797-826. doi: 10.1677/erc.1.01143. Endocr Relat Cancer. 2006. PMID: 16954431 Review.
-
Combining transfer of TTF-1 and Pax-8 gene: a potential strategy to promote radioiodine therapy of thyroid carcinoma.Cancer Gene Ther. 2012 Jun;19(6):402-11. doi: 10.1038/cgt.2012.13. Epub 2012 Apr 13. Cancer Gene Ther. 2012. PMID: 22498723
Cited by
-
The influence of thionamides on intra-thyroidal uptake of 131I during radioiodine-131 treatment of Graves' disease.Sci Rep. 2023 Dec 1;13(1):21190. doi: 10.1038/s41598-023-47228-z. Sci Rep. 2023. PMID: 38040820 Free PMC article.
-
Exploring the clinical utility of angioinvasion markers in papillary thyroid cancer: a literature review.Front Endocrinol (Lausanne). 2023 Nov 27;14:1261860. doi: 10.3389/fendo.2023.1261860. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38089632 Free PMC article. Review.
-
Genomic alterations in thyroid cancer: biological and clinical insights.Nat Rev Endocrinol. 2024 Feb;20(2):93-110. doi: 10.1038/s41574-023-00920-6. Epub 2023 Dec 4. Nat Rev Endocrinol. 2024. PMID: 38049644 Review.
-
Late-stage labeling of diverse peptides and proteins with iodine-125.J Pharm Anal. 2025 Jul;15(7):101198. doi: 10.1016/j.jpha.2025.101198. Epub 2025 Jan 17. J Pharm Anal. 2025. PMID: 40741338 Free PMC article. Review.
-
The role of miR-139-5p in radioiodine-resistant thyroid cancer.J Endocrinol Invest. 2023 Oct;46(10):2079-2093. doi: 10.1007/s40618-023-02059-7. Epub 2023 Mar 18. J Endocrinol Invest. 2023. PMID: 36933170 Free PMC article.
References
-
- Zhao L.M., Pang A.X. Iodine-131 treatment of thyroid cancer cells leads to suppression of cell proliferation followed by induction of cell apoptosis and cell cycle arrest by regulation of B-cell translocation gene 2-mediated JNK/NF-kappaB pathways. Braz. J. Med Biol. Res. Rev. Bras. Pesqui. Med. Biol. 2017;50:e5933. doi: 10.1590/1414-431x20165933. - DOI - PMC - PubMed
Publication types
Grants and funding
- SAF2015-69964-R/Ministerio de Economía y Competitividad
- RTI2018-099343-B-100/Ministerio de Ciencia, Innovación y Universidades
- PID2019-105303RB-I00/Ministerio de Ciencia, Innovación y Universidades
- 2014/0124/Asociación Española contra el Cáncer (AECC)
- CB16/12/00326/Centro de Investigación Biomédica en Red de Cáncer
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
