

Flow-related posterior cerebral artery aneurysms with internal carotid artery occlusions: An institutional series
- PMID: 33673757
- PMCID: PMC8493342
- DOI: 10.1177/15910199211001702
Flow-related posterior cerebral artery aneurysms with internal carotid artery occlusions: An institutional series
Abstract
Background: Aneurysm formation after internal carotid artery (ICA) occlusion has been described in animal models and human case series with alteration of cerebral blood flow dynamics considered an aetiological risk factor. Such de novo aneurysms have seldom been described in the posterior cerebral artery (PCA) with the majority observed in the anterior circulation collateral pathways.
Methods: We retrospectively reviewed our institutional database of posterior circulation aneurysms in patients with iatrogenic, atherosclerotic or congenital ICA occlusions. A comprehensive review of the online literature using the PubMed and Medline databases was performed to identify previous cases of PCA aneurysms that were considered 'flow-related'.
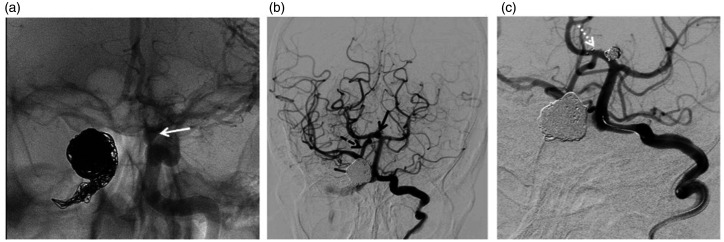
Results: We present five patients with symptomatic or ruptured PCA aneurysms with ICA occlusions. Age at presentation ranged from 21-58 and aneurysm size from 3-12 mm. All cases had angiographic evidence of posterior-anterior flow via the ipsilateral posterior communicating artery (PComA). The clinical presentation, diagnostic imaging and management strategies are further discussed. A literature review identified only two previous reported cases.
Conclusion: To our knowledge this is the first single centre series of posterior circulation aneurysms in patients with ICA occlusions that are considered to be 'flow-related.' The natural history of these rare lesions is unclear and the best management and surveillance strategy requires a patient-tailored approach by an experienced neurovascular team.
Keywords: Aneurysm; cerebral; flow-related; posterior circulation.
Conflict of interest statement
Figures




References
-
- Hassler O. Experimental carotid ligation followed by aneurysmal formation and other morphological changes in the circle of Willis. J Neurosurg 2009; 20: 1–7. DOI:10.3171/jns.1963.20.1.0001. - PubMed
-
- Dyste GN, Beck DW. De novo aneurysm formation following carotid ligation: case report and review of the literature. Neurosurgery 1989; 24: 88–92. DOI: 10.1227/00006123-198901000-00014. - PubMed
-
- Wang YY, Rosenfeld JV, Lyon SM, et al. Rapid development of a de novo intracranial aneurysm following carotid occlusion. J Clin Neurosci2008; 15: 324–330. DOI: 10.1016/j.jocn.2007.05.019. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
