

Association between components of the delirium syndrome and outcomes in hospitalised adults: a systematic review and meta-analysis
- PMID: 33673804
- PMCID: PMC7934253
- DOI: 10.1186/s12877-021-02095-z
Association between components of the delirium syndrome and outcomes in hospitalised adults: a systematic review and meta-analysis
Erratum in
-
Correction to: Association between components of the delirium syndrome and outcomes in hospitalised adults: a systematic review and meta-analysis.BMC Geriatr. 2021 Sep 9;21(1):490. doi: 10.1186/s12877-021-02419-z. BMC Geriatr. 2021. PMID: 34503451 Free PMC article. No abstract available.
Abstract
Background: Delirium is a heterogeneous syndrome with inattention as the core feature. There is considerable variation in the presence and degree of other symptom domains such as altered arousal, psychotic features and global cognitive dysfunction. Delirium is independently associated with increased mortality, but it is unclear whether individual symptom domains of delirium have prognostic importance. We conducted a systematic review and meta-analysis of studies in hospitalised adults in general settings to identify the relationship between symptom domains of delirium and outcomes. (PROSPERO: CRD42018093935).
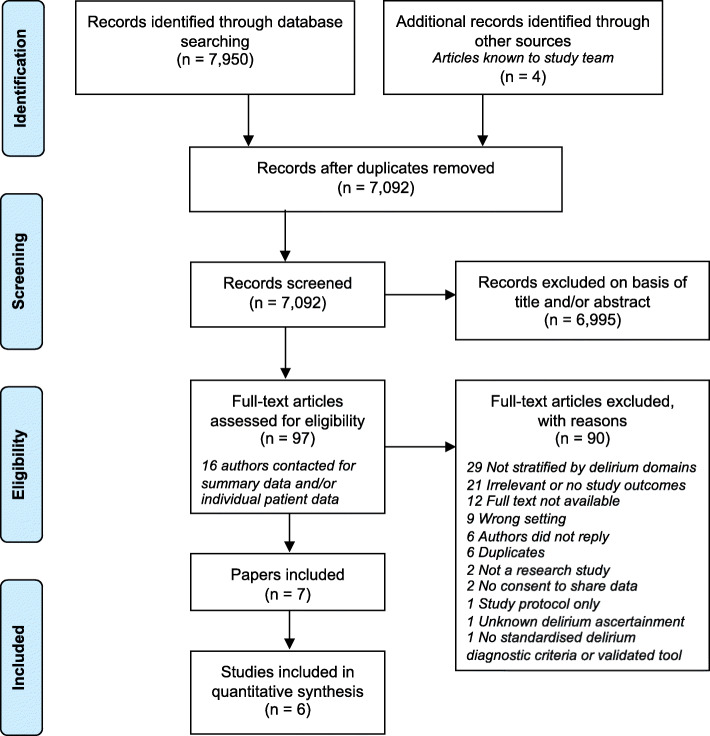
Methods: We searched MEDLINE, EMBASE, PsycINFO, CINAHL, clinicaltrials.gov and the Cochrane Central Register of Controlled Trials from inception to November 2019. We included studies of hospitalised adults that reported associations between symptom domains of delirium and 30-day mortality (primary outcome), and other outcomes including mortality at other time points, length of stay, and dementia. Reviewer pairs independently screened articles, extracted data, and assessed risk of bias (Risk of Bias Assessment tool for Non-randomized Studies) and quality of evidence using the Grading of Recommendations, Assessment, Development and Evaluation framework. We performed random-effects meta-analyses stratified by delirium domain where possible.
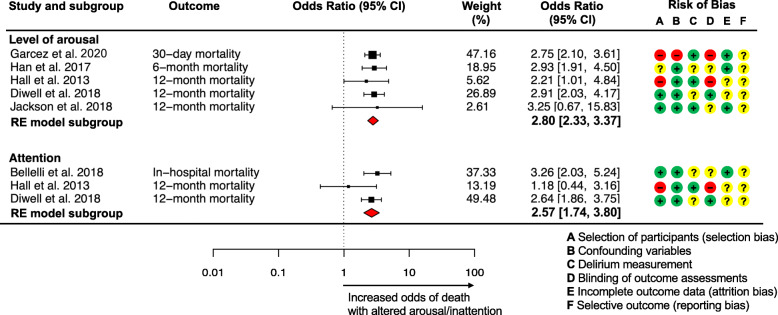
Results: From 7092 citations we included 6 studies (6002 patients, 1112 with delirium). Higher mortality (ranging from in-hospital to follow-up beyond 12 months) was associated with altered arousal (pooled Odds Ratio (OR) 2.80, 95% Confidence Interval (CI) 2.33-3.37; moderate-quality evidence), inattention (pooled OR 2.57, 95% CI 1.74-3.80; low-quality evidence), and in single studies with disorientation, memory deficits and disorganised thoughts. Risk of bias varied across studies but was moderate-to-high overall, mainly due to selection bias, lack of blinding of assessments and unclear risk of selective outcome reporting. We found no studies on the association between psychotic features, visuospatial deficits or affective disturbances in delirium and outcomes, or studies reporting non-mortality outcomes.
Conclusions: Few studies have related symptom domains of delirium to outcomes, but the available evidence suggests that altered arousal and inattention in delirium are associated with higher mortality than normal arousal and attention in people with or without delirium. Measurable symptom domains of delirium may have value in predicting survival and stratifying patients for treatment. We recommend that future delirium studies report outcomes by symptom domain.
Keywords: Altered mental status; Arousal; Attention; Delirium; Mortality; Systematic review.
Conflict of interest statement
The authors declare no competing interest.
Figures
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Cognitive training for people with mild to moderate dementia.Cochrane Database Syst Rev. 2019 Mar 25;3(3):CD013069. doi: 10.1002/14651858.CD013069.pub2. Cochrane Database Syst Rev. 2019. PMID: 30909318 Free PMC article.
-
Interventions for preventing intensive care unit delirium in adults.Cochrane Database Syst Rev. 2018 Nov 23;11(11):CD009783. doi: 10.1002/14651858.CD009783.pub2. Cochrane Database Syst Rev. 2018. PMID: 30484283 Free PMC article.
-
Interventions for preventing delirium in older people in institutional long-term care.Cochrane Database Syst Rev. 2019 Apr 23;4(4):CD009537. doi: 10.1002/14651858.CD009537.pub3. Cochrane Database Syst Rev. 2019. PMID: 31012953 Free PMC article.
-
Computerised cognitive training for 12 or more weeks for maintaining cognitive function in cognitively healthy people in late life.Cochrane Database Syst Rev. 2020 Feb 27;2(2):CD012277. doi: 10.1002/14651858.CD012277.pub3. Cochrane Database Syst Rev. 2020. PMID: 32104914 Free PMC article.
Cited by
-
Delirium in Frail Older Adults.Ann Geriatr Med Res. 2021 Sep;25(3):150-159. doi: 10.4235/agmr.21.0082. Epub 2021 Aug 30. Ann Geriatr Med Res. 2021. PMID: 34455754 Free PMC article.
-
Inflammatory biomarkers and delirium: a Mendelian randomization study.Front Aging Neurosci. 2023 Aug 15;15:1221272. doi: 10.3389/fnagi.2023.1221272. eCollection 2023. Front Aging Neurosci. 2023. PMID: 37649721 Free PMC article.
-
Phenotypes and subphenotypes of delirium: a review of current categorisations and suggestions for progression.Crit Care. 2021 Sep 15;25(1):334. doi: 10.1186/s13054-021-03752-w. Crit Care. 2021. PMID: 34526093 Free PMC article. Review.
-
The effect of baseline cognition and delirium on long-term cognitive impairment and mortality: a prospective population-based study.Lancet Healthy Longev. 2022 Apr;3(4):e232-e241. doi: 10.1016/S2666-7568(22)00013-7. Lancet Healthy Longev. 2022. PMID: 35382093 Free PMC article.
-
Nurses' competence in recognition and management of delirium in older patients: development and piloting of a self-assessment tool.BMC Geriatr. 2022 Nov 19;22(1):879. doi: 10.1186/s12877-022-03573-8. BMC Geriatr. 2022. PMID: 36402941 Free PMC article.
References
-
- Reynish EL, Hapca SM, De Souza N, Cvoro V, Donnan PT, Guthrie B. Epidemiology and outcomes of people with dementia, delirium, and unspecified cognitive impairment in the general hospital: prospective cohort study of 10,014 admissions. BMC Med. 2017;15:140. doi: 10.1186/s12916-017-0899-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
