

Ventilation strategies for front of neck airway rescue: an in silico study
- PMID: 33674075
- PMCID: PMC8216300
- DOI: 10.1016/j.bja.2021.01.030
Ventilation strategies for front of neck airway rescue: an in silico study
Abstract
Background: During induction of general anaesthesia a 'cannot intubate, cannot oxygenate' (CICO) situation can arise, leading to severe hypoxaemia. Evidence is scarce to guide ventilation strategies for small-bore emergency front of neck airways that ensure effective oxygenation without risking lung damage and cardiovascular depression.
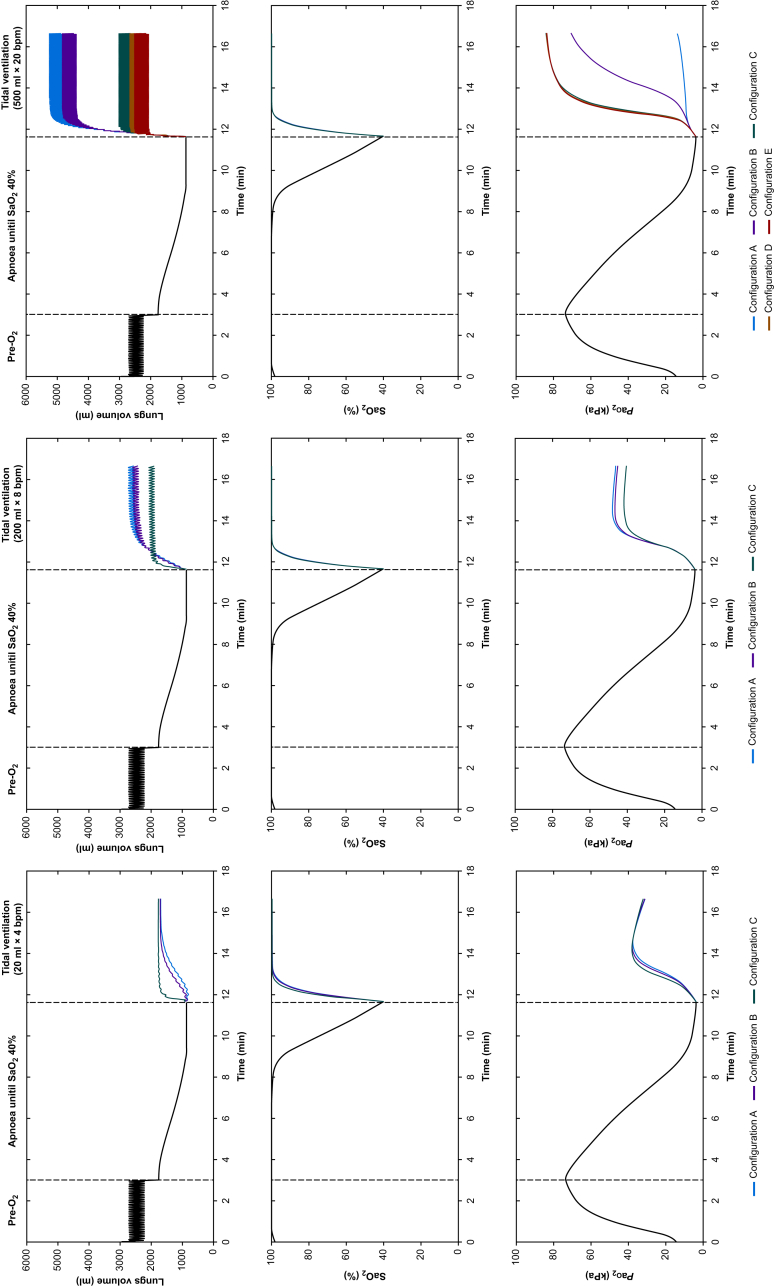
Methods: Fifty virtual subjects were configured using a high-fidelity computational model of the cardiovascular and pulmonary systems. Each subject breathed 100% oxygen for 3 min and then became apnoeic, with an obstructed upper airway. When arterial haemoglobin oxygen saturation reached 40%, front of neck airway access was simulated with various configurations. We examined the effect of several ventilation strategies on re-oxygenation, pulmonary pressures, cardiovascular function, and oxygen delivery.
Results: Re-oxygenation was achieved in all ventilation strategies. Smaller airway configurations led to dynamic hyperinflation for a wide range of ventilation strategies. This effect was absent in airways with larger internal diameter (≥3 mm). Intrapulmonary pressures increased quickly to supra-physiological values with the smallest airways, resulting in pronounced cardio-circulatory depression (cardiac output <3 L min-1 and mean arterial pressure <60 mm Hg), impeding oxygen delivery (<600 ml min-1). Limiting tidal volume (≤200 ml) and ventilatory frequency (≤8 bpm) for smaller diameter cannulas reduced dynamic hyperinflation and gas trapping, preventing cardiovascular depression.
Conclusions: Dynamic hyperinflation can be demonstrated for a wide range of front of neck airway cannulae when the upper airway is obstructed. When using small-bore cannulae in a CICO situation, ventilation strategies should be chosen that prevent gas trapping to prevent severe adverse events including cardio-circulatory depression.
Keywords: airway management; airway obstruction; apnoea; cannot intubate; cannot oxygenate; front of neck airway; oxygenation simulation.
Copyright © 2021 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declarations of interest JGH is associate editor-in-chief of the British Journal of Anaesthesia. JGH accepts fees for the provision of advice to the police, crown prosecution service, coroners and solicitors. The other authors have no conflicts to declare.
Figures






Comment in
-
New evidence to inform decisions and guidelines in difficult airway management.Br J Anaesth. 2021 Jun;126(6):1094-1097. doi: 10.1016/j.bja.2021.03.003. Epub 2021 Apr 6. Br J Anaesth. 2021. PMID: 33836852 No abstract available.
References
-
- Duggan L.V., Ballantyne Scott B., Law J.A., Morris I.R., Murphy M.F., Griesdale D.E. Transtracheal jet ventilation in the ‘can’t intubate can’t oxygenate’ emergency: a systematic review. Br J Anaesth. 2016;117:i28–38. - PubMed
-
- Cook T.M., Woodall N., Frerk C. Major complications of airway management in the UK: results of the fourth national audit project of the royal college of anaesthetists and the difficult airway society. Part 1. Anaesthesia. Br J Anaesth. 2011;106:617–631. - PubMed
-
- Dworkin R., Benumof J.L., Benumof R., Karagianes T.G. The effective tracheal diameter that causes air trapping during jet ventilation. J Cardiothorac Anesth. 1990;4:731–736. - PubMed
-
- Blanch L., Bernabé F., Lucangelo U. Measurement of air trapping, intrinsic positive end-expiratory pressure, and dynamic hyperinflation in mechanically ventilated patients. Respir Care. 2005;50:110–124. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
