

A Cost-Effectiveness Analysis of Nivolumab Plus Ipilimumab Versus Pembrolizumab Plus Axitinib and Versus Avelumab Plus Axitinib in First-Line Treatment of Advanced Renal Cell Carcinoma
- PMID: 33674224
- PMCID: PMC9643032
- DOI: 10.1016/j.clgc.2021.01.009
A Cost-Effectiveness Analysis of Nivolumab Plus Ipilimumab Versus Pembrolizumab Plus Axitinib and Versus Avelumab Plus Axitinib in First-Line Treatment of Advanced Renal Cell Carcinoma
Abstract
Background: There now exist several viable first-line treatment options for metastatic renal cell carcinoma, making the choice of initial therapy difficult. Considering metrics other than patient factors may be necessary to select the most appropriate therapy. We aimed to assess the cost-effectiveness of the three combination therapies currently approved in treatment-naïve advanced or metastatic renal cell carcinoma-nivolumab + ipilimumab (NI), pembrolizumab + axitinib (PA), and avelumab + axitinib (AA)-from a US payer perspective.
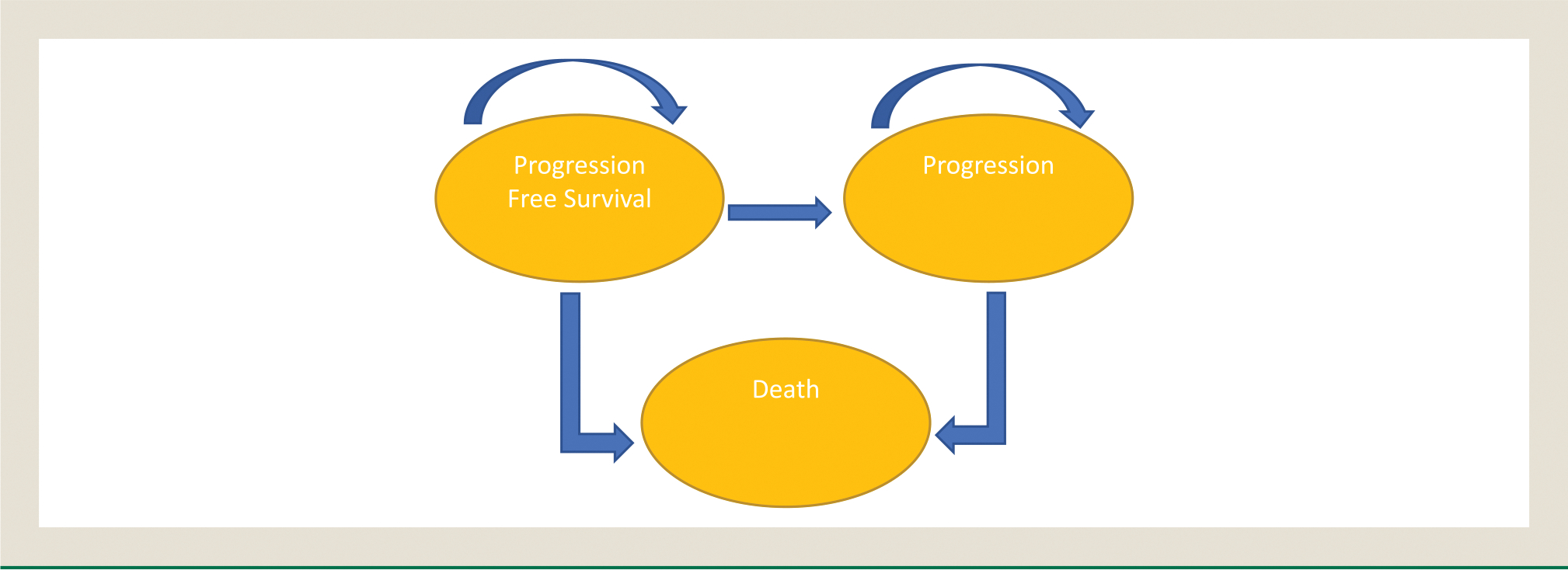
Patients and methods: Our analysis was performed based on previously obtained data derived from progression-free survival and overall survival curves from CheckMate 214, KEYNOTE 426, and JAVELIN Renal 101.
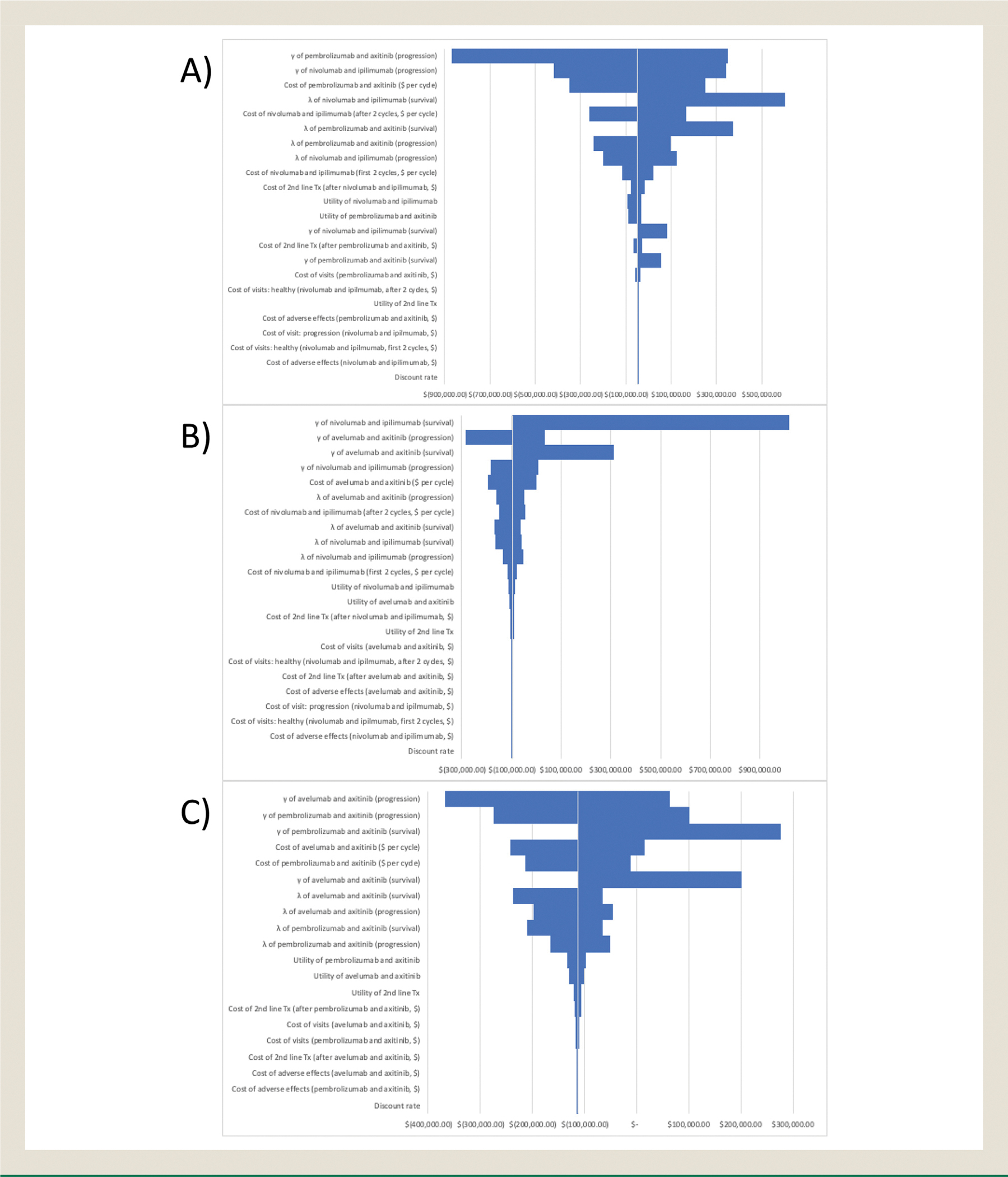
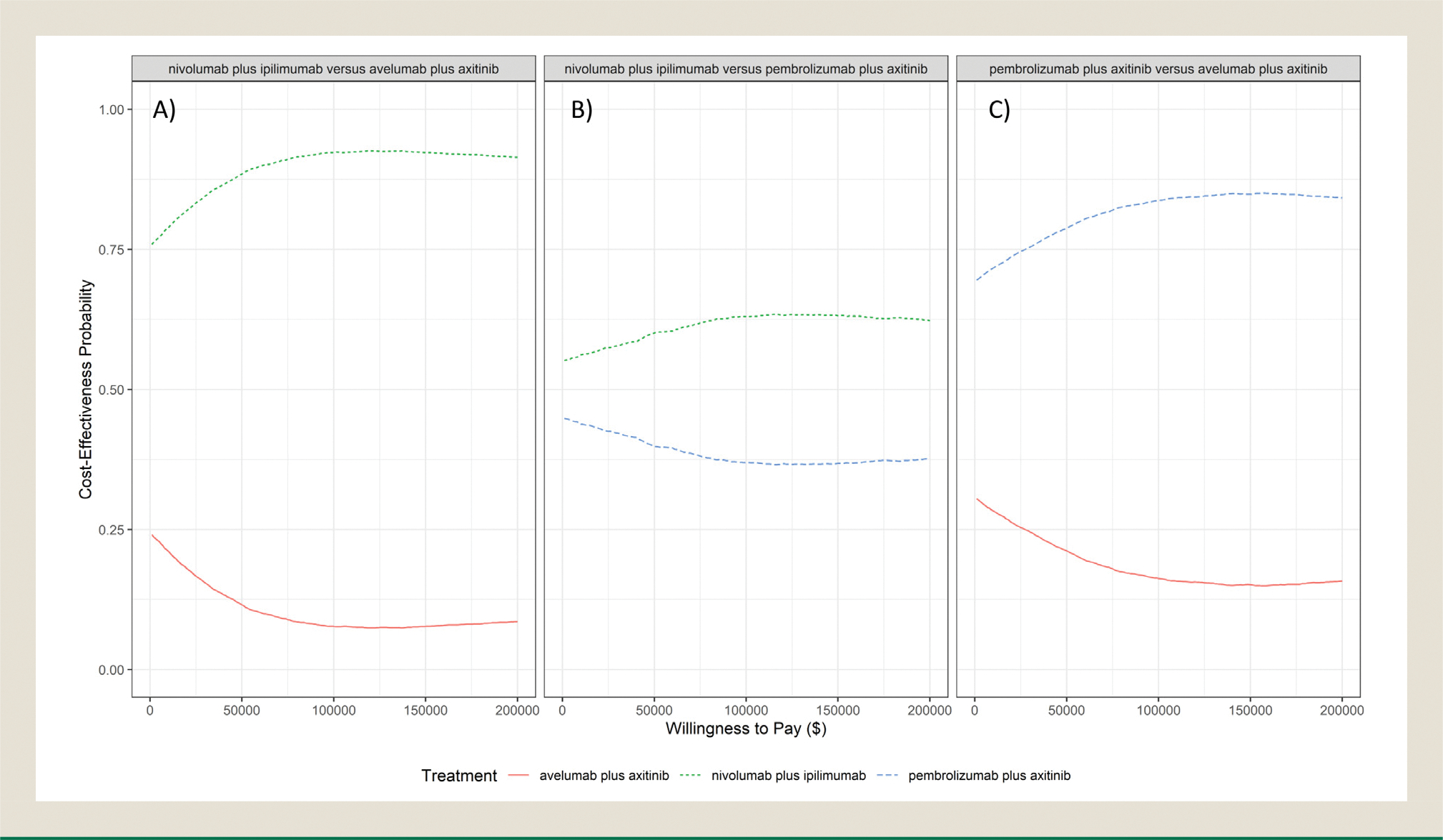
Results: The total costs of each treatment were found to be $437,556.12 for NI, $450,597.15 for PA, and $542,882.34 for AA, with quality-adjusted life-year (QALY) values of 4.04, 3.77, and 2.95 for each combination, respectively. The incremental cost-effectiveness ratio (ICER) of NI versus PA was ($47,504.73/QALY); for NI versus AA, it was ($96,533.11/QALY); for PA versus AA, it was ($113,015.87/QALY). Net health benefit scaled against a willingness-to-pay threshold of $150,000 per QALY was positive for NI versus PA at 0.36 and versus AA at 1.79, and this index was also positive for PA versus AA at 1.43, indicating that the additional value of these therapies versus their alternatives is greater than the extra cost.
Conclusion: NI was found to be the most cost-effective treatment option compared with the other considered therapies. PA was found to be cost effective compared to AA. When patient factors such as social issues and pre-existing conditions do not dictate their first-line therapy, clinicians may use this additional information to make financially conscious choices.
Keywords: Cost–benefit analysis; Health care costs; Immunotherapy; Monoclonal antibodies; Protein tyrosine kinases.
Copyright © 2021. Published by Elsevier Inc.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Albiges L, Tannir N, Burotto M, et al. 711P nivolumab + ipilimumab (N+I) vs sunitinib (S) for first-line treatment of advanced renal cell carcinoma (aRCC) in CheckMate 214: 4-year follow-up and subgroup analysis of patients (pts) without nephrectomy. Ann Oncol. 2020;31:S559–S560.
-
- US Food and Drug Administration. FDA approves nivolumab plus ipilimumab combination for intermediate- or poor-risk advanced renal cell carcinoma. Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-appro.... Accessed February 22, 2021.
-
- National Comprehensive Cancer Network. NCCN Clinical Guidelines in Oncology. Available at: https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed February 22, 2021.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
