

Evaluation of Specimen Types and Saliva Stabilization Solutions for SARS-CoV-2 Testing
- PMID: 33674284
- PMCID: PMC8091857
- DOI: 10.1128/JCM.01418-20
Evaluation of Specimen Types and Saliva Stabilization Solutions for SARS-CoV-2 Testing
Abstract
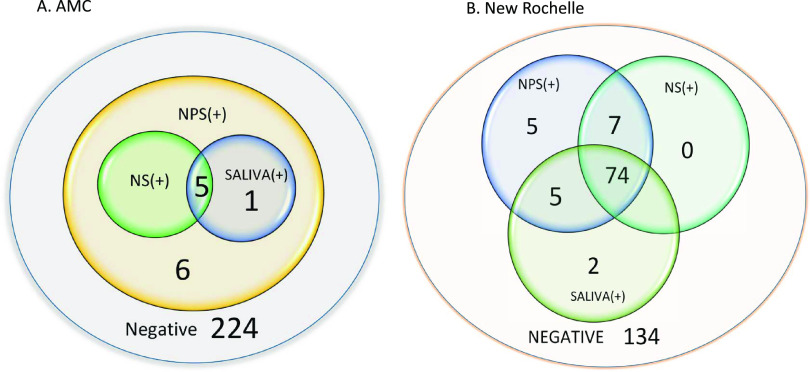
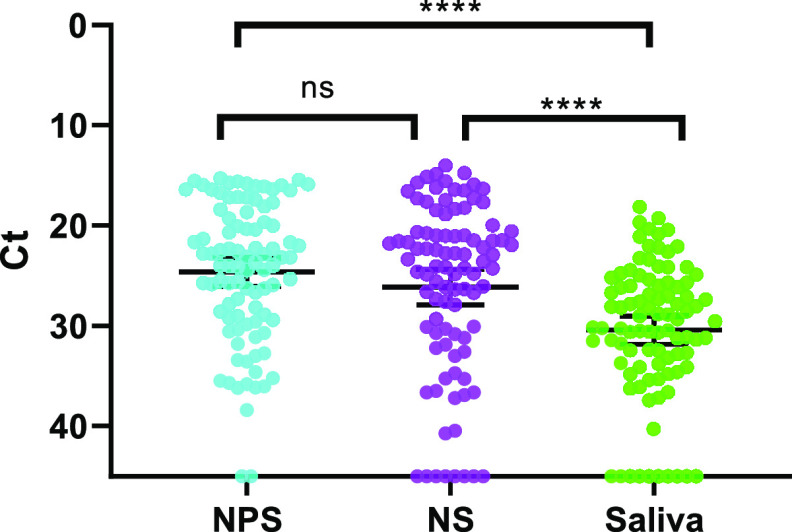
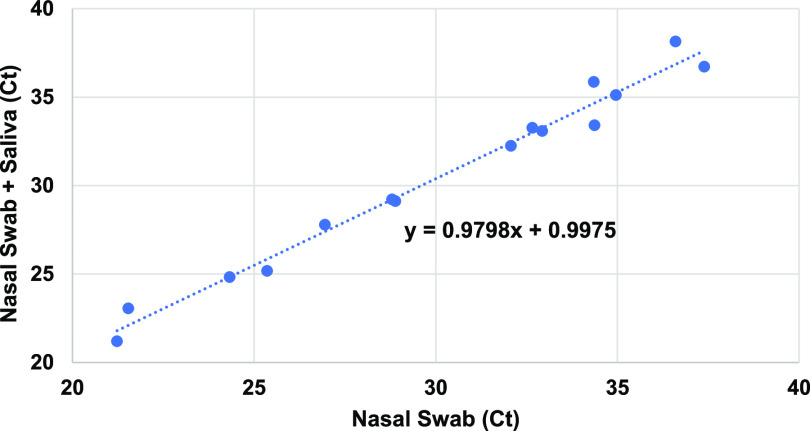
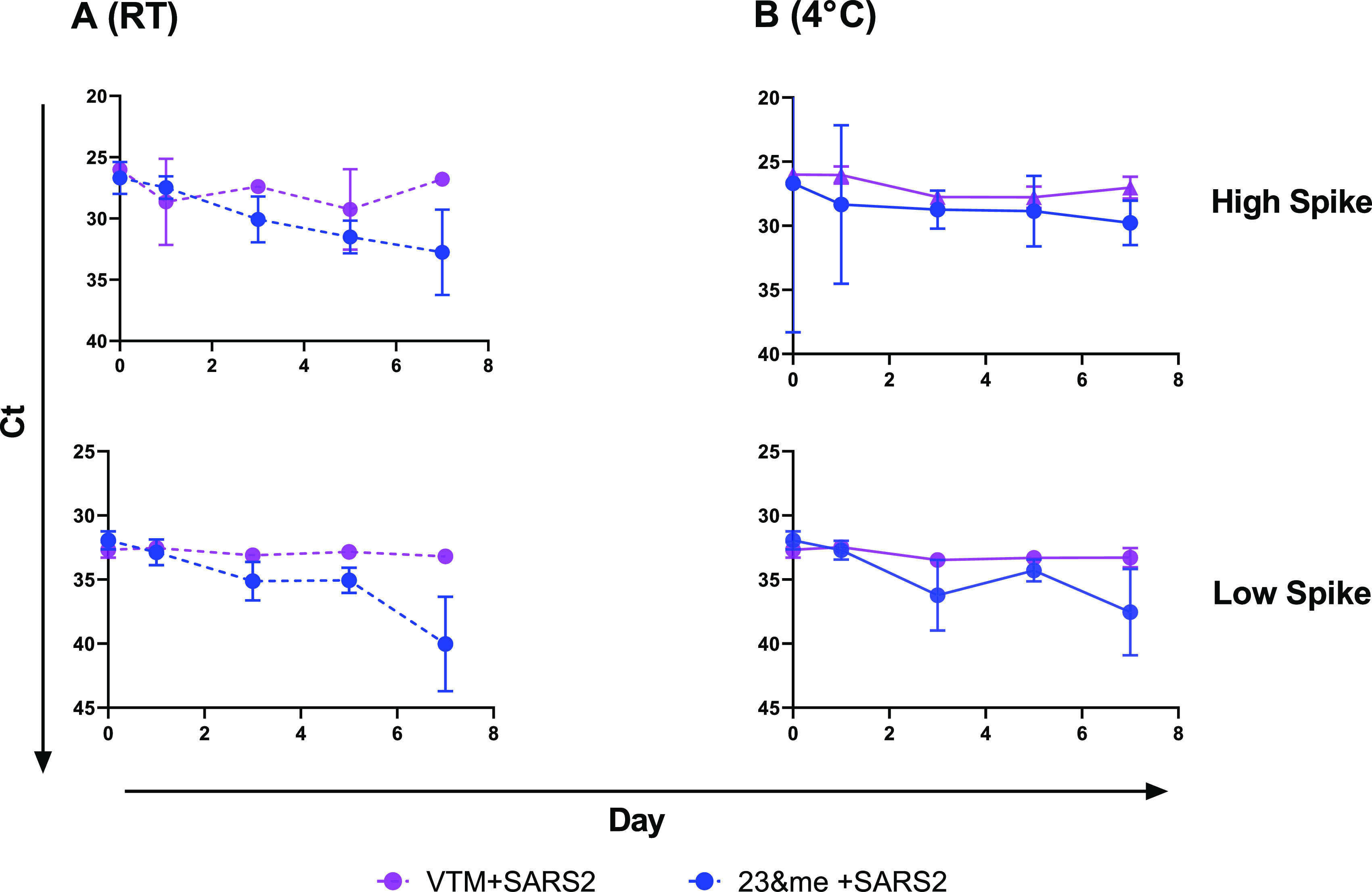
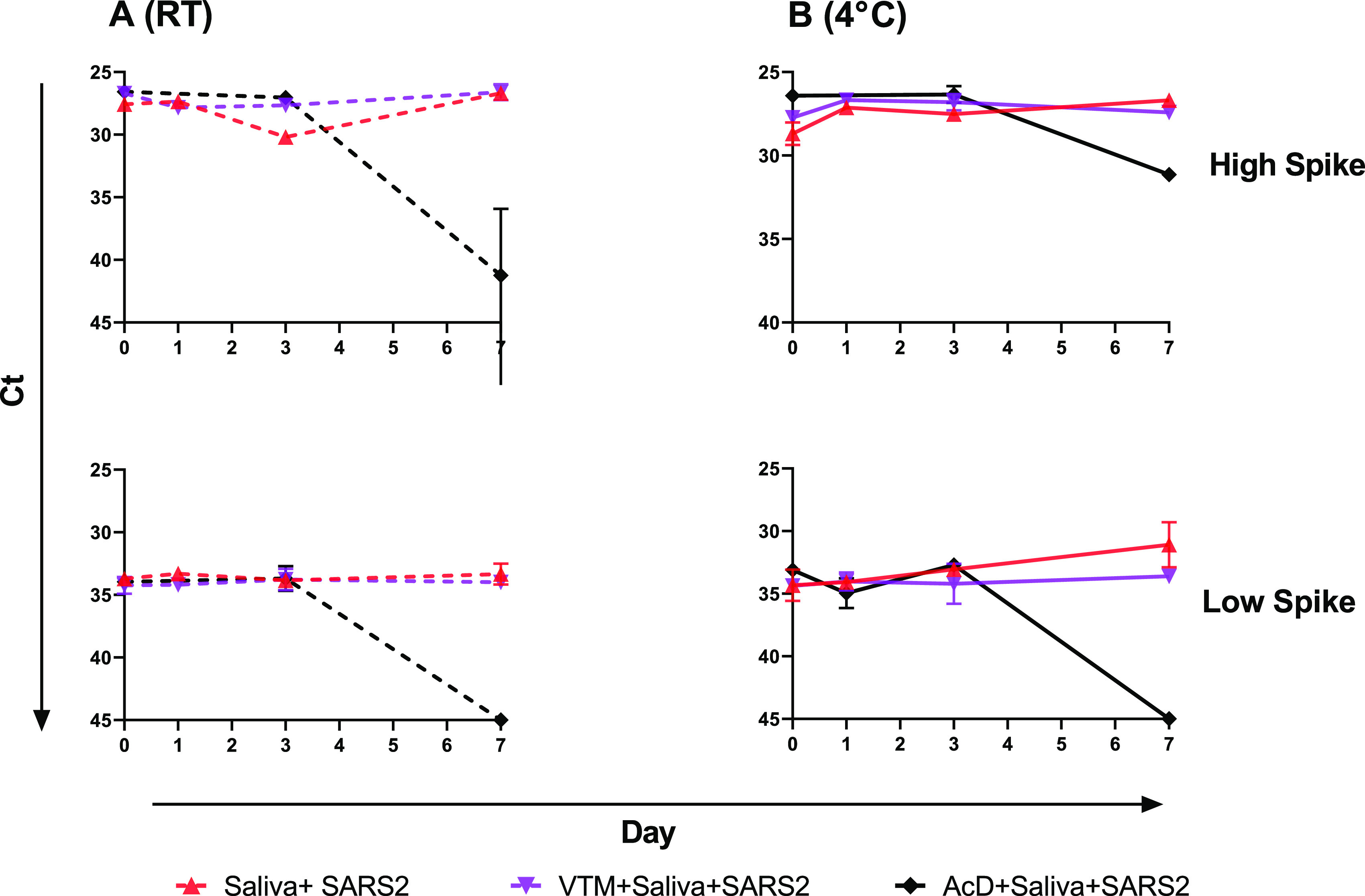
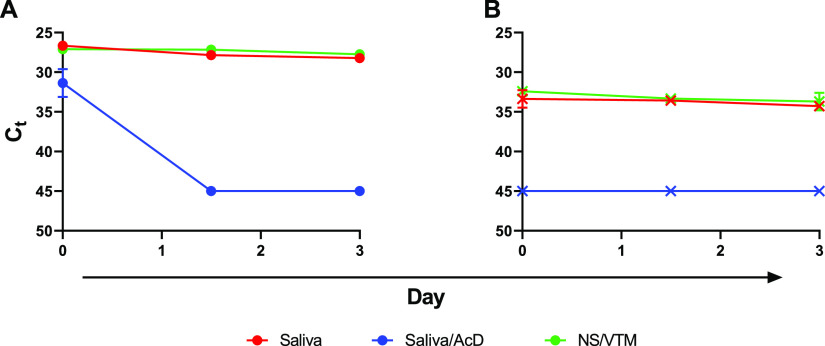
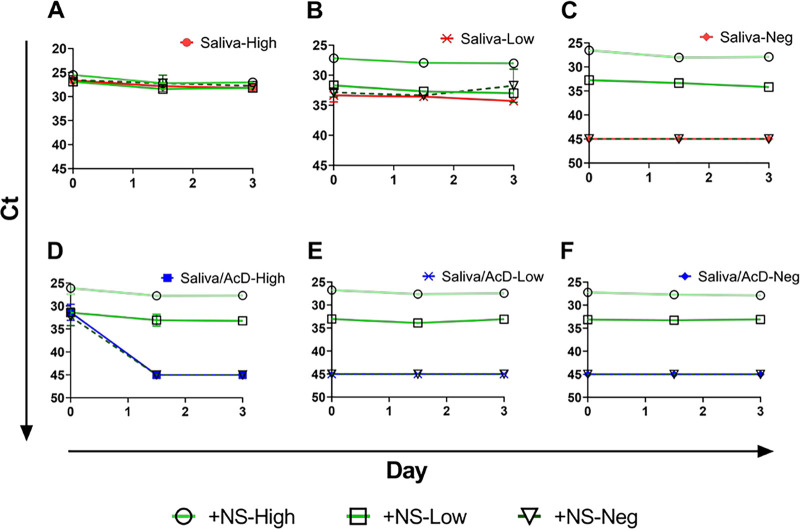
Identifying SARS-CoV-2 infections through aggressive diagnostic testing remains critical to tracking and curbing the spread of the COVID-19 pandemic. Collection of nasopharyngeal swabs (NPS), the preferred sample type for SARS-CoV-2 detection, has become difficult due to the dramatic increase in testing and consequent supply strain. Therefore, alternative specimen types have been investigated that provide similar detection sensitivity with reduced health care exposure and the potential for self-collection. In this study, the detection sensitivity of SARS-CoV-2 in nasal swabs (NS) and saliva was compared to that of NPS using matched specimens from two outpatient cohorts in New York State (total n = 463). The first cohort showed only a 5.4% positivity, but the second cohort (n = 227) had a positivity rate of 41%, with sensitivity in NPS, NS, and saliva of 97.9%, 87.1%, and 87.1%, respectively. Whether the reduced sensitivity of NS or saliva is acceptable must be assessed in the settings where they are used. However, we sought to improve on it by validating a method to mix the two sample types, as the combination of nasal swab and saliva resulted in 94.6% SARS-CoV-2 detection sensitivity. Spiking experiments showed that combining them did not adversely affect the detection sensitivity in either. Virus stability in saliva was also investigated, with and without the addition of commercially available stabilizing solutions. The virus was stable in saliva at both 4°C and room temperature for up to 7 days. The addition of stabilizing solutions did not enhance stability and, in some situations, reduced detectable virus levels.
Keywords: COVID-19; nasal swab; nasopharyngeal swab; saliva; sample type.
Copyright © 2021 American Society for Microbiology.
Figures
References
-
- Patel R, Babady E, Theel ES, Storch GA, Pinsky BA, St George K, Smith TC, Bertuzzi S. 2020. Report from the American Society for Microbiology COVID-19 International Summit, 23 March 2020: value of diagnostic testing for SARS-CoV-2/COVID-19. mBio 11:e00722-20. 10.1128/mBio.00722-20. - DOI - PMC - PubMed
-
- Pere H, Podglajen I, Wack M, Flamarion E, Mirault T, Goudot G, Hauw-Berlemont C, Le L, Caudron E, Carrabin S, Rodary J, Ribeyre T, Belec L, Veyer D. 2020. Nasal swab sampling for SARS-CoV-2: a convenient alternative in times of nasopharyngeal swab shortage. J Clin Microbiol 58:e00721-20. 10.1128/JCM.00721-20. - DOI - PMC - PubMed
-
- Rowan NJ, Laffey JG. 2020. Challenges and solutions for addressing critical shortage of supply chain for personal and protective equipment (PPE) arising from coronavirus disease (COVID19) pandemic–case study from the Republic of Ireland. Sci Total Environ 725:138532. 10.1016/j.scitotenv.2020.138532. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
