

Colorectal cancer risk following polypectomy in a multicentre, retrospective, cohort study: an evaluation of the 2020 UK post-polypectomy surveillance guidelines
- PMID: 33674342
- PMCID: PMC8588296
- DOI: 10.1136/gutjnl-2020-323411
Colorectal cancer risk following polypectomy in a multicentre, retrospective, cohort study: an evaluation of the 2020 UK post-polypectomy surveillance guidelines
Abstract
Objective: Colonoscopy surveillance aims to reduce colorectal cancer (CRC) incidence after polypectomy. The 2020 UK guidelines recommend surveillance at 3 years for 'high-risk' patients with ≥2 premalignant polyps (PMPs), of which ≥1 is 'advanced' (serrated polyp (or adenoma) ≥10 mm or with (high-grade) dysplasia); ≥5 PMPs; or ≥1 non-pedunculated polyp ≥20 mm; 'low-risk' patients without these findings are instead encouraged to participate in population-based CRC screening. We examined the appropriateness of these risk classification criteria and recommendations.
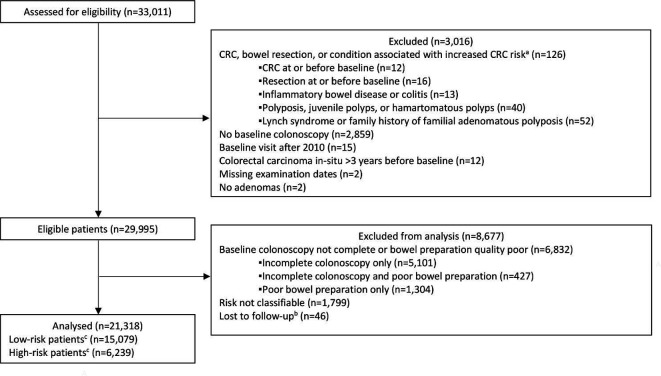
Design: Retrospective analysis of patients who underwent colonoscopy and polypectomy mostly between 2000 and 2010 at 17 UK hospitals, followed-up through 2017. We examined CRC incidence by baseline characteristics, risk group and number of surveillance visits using Cox regression, and compared incidence with that in the general population using standardised incidence ratios (SIRs).
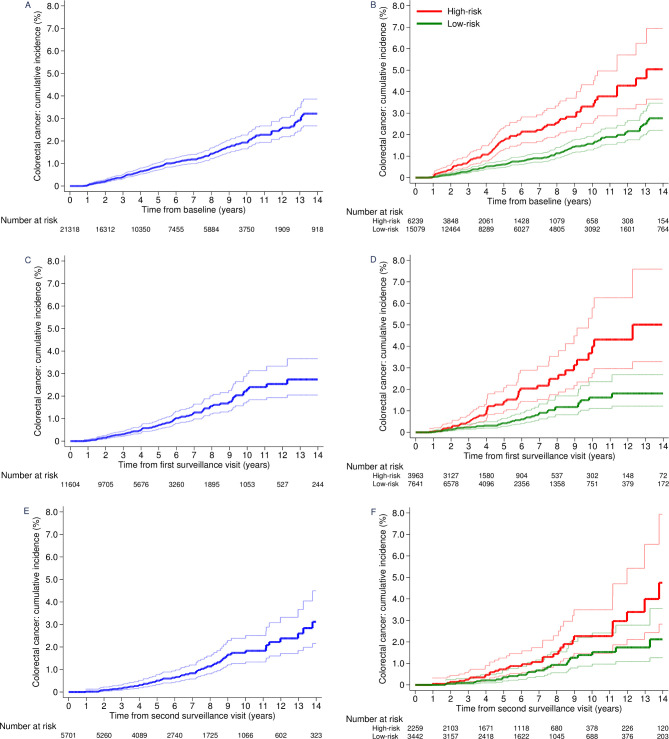
Results: Among 21 318 patients, 368 CRCs occurred during follow-up (median: 10.1 years). Baseline CRC risk factors included age ≥55 years, ≥2 PMPs, adenomas with tubulovillous/villous/unknown histology or high-grade dysplasia, proximal polyps and a baseline visit spanning 2-90 days. Compared with the general population, CRC incidence without surveillance was higher among those with adenomas with high-grade dysplasia (SIR 1.74, 95% CI 1.21 to 2.42) or ≥2 PMPs, of which ≥1 was advanced (1.39, 1.09 to 1.75). For low-risk (71%) and high-risk (29%) patients, SIRs without surveillance were 0.75 (95% CI 0.63 to 0.88) and 1.30 (1.03 to 1.62), respectively; for high-risk patients after first surveillance, the SIR was 1.22 (0.91 to 1.60).
Conclusion: These guidelines accurately classify post-polypectomy patients into those at high risk, for whom one surveillance colonoscopy appears appropriate, and those at low risk who can be managed by non-invasive screening.
Keywords: colonoscopy; colorectal adenomas; colorectal cancer; colorectal cancer screening; surveillance.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: AJC, as Chief Investigator, was the recipient of all the funding. MDR reports personal fees from Swiss SCWeb AG, Pentax, and Norgine, and a grant from Olympus, outside the submitted work.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical