

Targeted Antibiotics for Trachoma: A Cluster-Randomized Trial
- PMID: 33674869
- PMCID: PMC8442777
- DOI: 10.1093/cid/ciab193
Targeted Antibiotics for Trachoma: A Cluster-Randomized Trial
Abstract
Background: Current guidelines recommend community-wide mass azithromycin for trachoma, but a targeted treatment strategy could reduce the volume of antibiotics required.
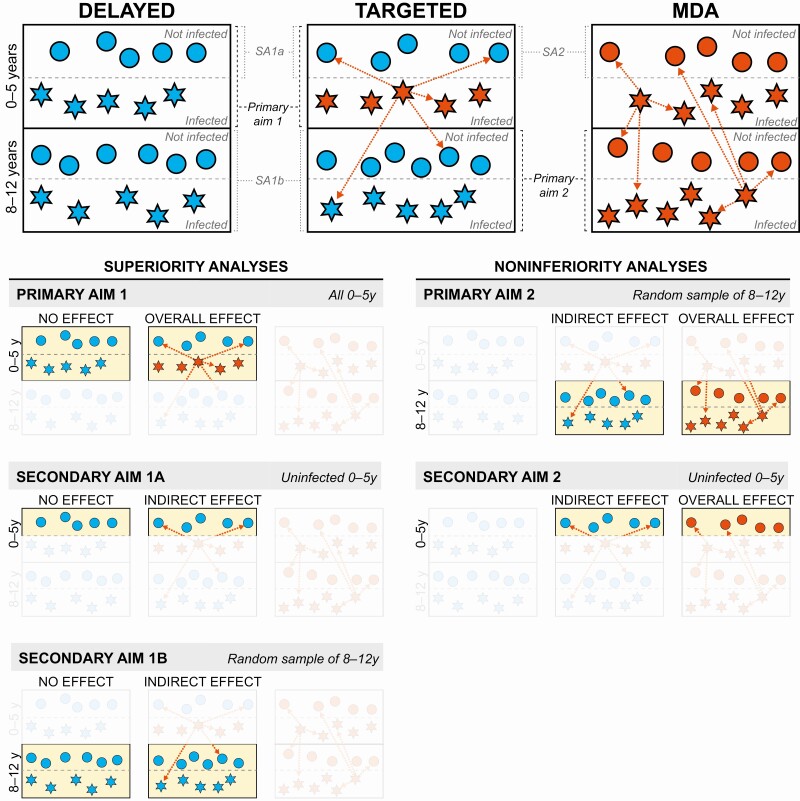
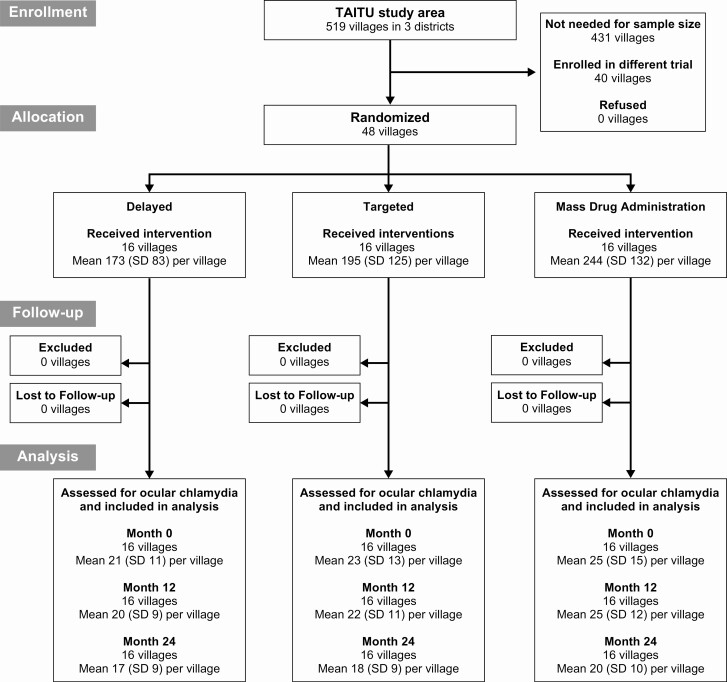
Methods: In total, 48 Ethiopian communities were randomized to mass, targeted, or delayed azithromycin distributions. In the targeted arm, only children aged 6 months to 5 years with evidence of ocular chlamydia received azithromycin, distributed thrice over the following year. The primary outcome was ocular chlamydia at months 12 and 24, comparing the targeted and delayed arms (0-5 year-olds, superiority analysis) and the targeted and mass azithromycin arms (8-12 year-olds, noninferiority analysis, 10% noninferiority margin).
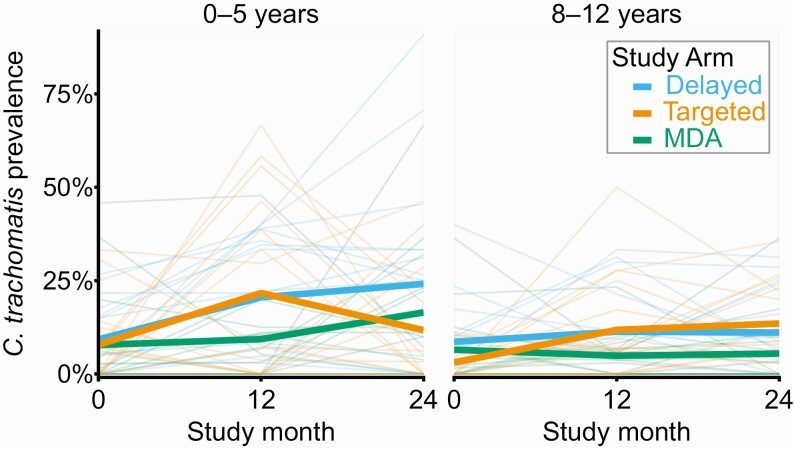
Results: At baseline, the mean prevalence of ocular chlamydia in the 3 arms ranged from 7% to 9% among 0-5 year-olds and from 3% to 9% among 8-12 year-olds. Averaged across months 12-24, the mean prevalence of ocular chlamydia among 0-5 year-olds was 16.7% (95% confidence interval [CI]: 9.0%-24.4%) in the targeted arm and 22.3% (95% CI: 11.1%-33.6%) in the delayed arm (P = .61). The final mean prevalence of ocular chlamydia among 8-12 year-olds was 13.5% (95% CI: 7.9%-19.1%) in the targeted arm and 5.5% (95% CI: 0.3%-10.7%) in the mass treatment arm (adjusted risk difference 8.5 percentage points [pp] higher in the targeted arm, 95% CI: 0.9 pp-16.1 pp higher).
Conclusions: Antibiotic treatments targeted to infected preschool children did not result in significantly less ocular chlamydia infections compared with untreated communities and did not meet noninferiority criteria relative to mass azithromycin distributions. Targeted approaches may require treatment of a broader segment of the population in areas with hyperendemic trachoma.
Keywords: Africa; antibacterial agents; chlamydia; mass drug administration; trachoma.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Solomon AW, World Health Organization , London School of Hygiene and Tropical Medicine, International Trachoma Initiative. Trachoma control: a guide for programme managers. Geneva: World Health Organization, 2006.
-
- Solomon AW, Holland MJ, Burton MJ, et al. . Strategies for control of trachoma: observational study with quantitative PCR. Lancet 2003; 362:198–204. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
