

An Eastern Association for the Surgery of Trauma multicenter trial examining prehospital procedures in penetrating trauma patients
- PMID: 33675330
- PMCID: PMC8216597
- DOI: 10.1097/TA.0000000000003151
An Eastern Association for the Surgery of Trauma multicenter trial examining prehospital procedures in penetrating trauma patients
Abstract
Background: Prehospital procedures (PHP) by emergency medical services (EMS) are performed regularly in penetrating trauma patients despite previous studies demonstrating no benefit. We sought to examine the influence of PHPs on outcomes in penetrating trauma patients in urban locations where transport to trauma center is not prolonged. We hypothesized that patients without PHPs would have better outcomes than those undergoing PHP.
Methods: This was an Eastern Association for the Surgery of Trauma-sponsored, multicenter, prospective, observational trial of adults (18+ years) with penetrating trauma to the torso and/or proximal extremity presenting at 25 urban trauma centers. The impact of PHPs and transport mechanism on in-hospital mortality were examined.
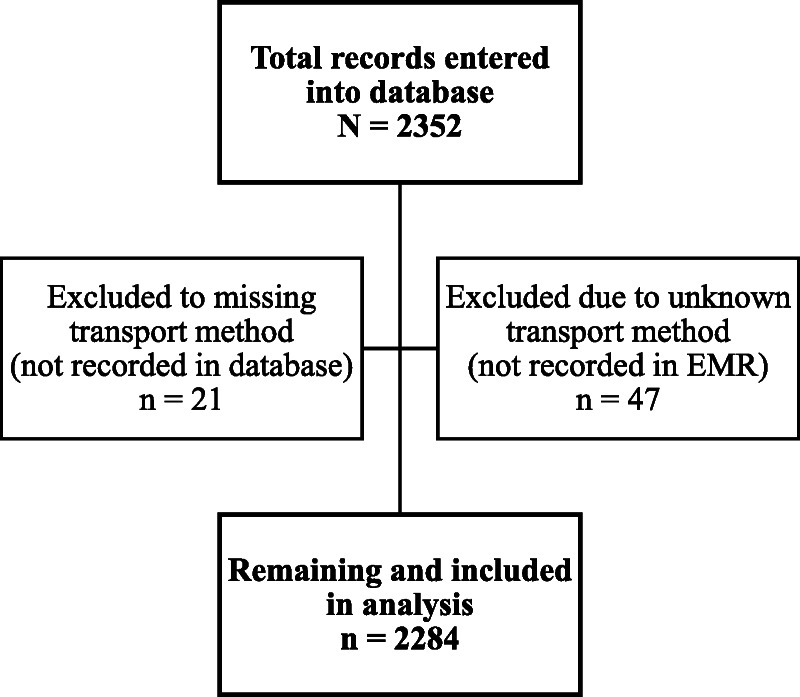
Results: Of 2,284 patients included, 1,386 (60.7%) underwent PHP. The patients were primarily Black (n = 1,527, 66.9%) males (n = 1,986, 87.5%) injured by gunshot wound (n = 1,510, 66.0%) with 34.1% (n = 726) having New Injury Severity Score of ≥16. A total of 1,427 patients (62.5%) were transported by Advanced Life Support EMS, 17.2% (n = 392) by private vehicle, 13.7% (n = 312) by police, and 6.7% (n = 153) by Basic Life Support EMS. Of the PHP patients, 69.1% received PHP on scene, 59.9% received PHP in route, and 29.0% received PHP both on scene and in route. Initial scene vitals differed between groups, but initial emergency department vitals did not. Receipt of ≥1 PHP increased mortality odds (odds ratio [OR], 1.36; 95% confidence interval [CI], 1.01-1.83; p = 0.04). Logistic regression showed increased mortality with each PHP, whether on scene or during transport. Subset analysis of specific PHP revealed that intubation (OR, 10.76; 95% CI, 4.02-28.78; p < 0.001), C-spine immobilization (OR, 5.80; 95% CI, 1.85-18.26; p < 0.01), and pleural decompression (OR, 3.70; 95% CI, 1.33-10.28; p = 0.01) had the highest odds of mortality after adjusting for multiple variables.
Conclusion: Prehospital procedures in penetrating trauma patients impart no survival advantage and may be harmful in urban settings, even when performed during transport. Therefore, PHP should be forgone in lieu of immediate transport to improve patient outcomes.
Level of evidence: Prognostic, level III.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Surgery of Trauma.
Figures

References
-
- Seamon MJ, Doane SM, Gaughan JP, Kulp H, D’Andrea AP, Pathak AS, Santora TA, Goldberg AJ, Wydro GC. Prehospital interventions for penetrating trauma victims: a prospective comparison between advanced life support and basic life support. Injury. 2013;44(5):634–638. - PubMed
-
- Haut ER, Kalish BT, Cotton BA, EFron DT, Haider AH, Stevens KA, Kieninger AN, Cornwell EE, 3rd, Chang DC. Prehospital intravenous fluid administration is associated with higher mortality in trauma patients: a National Trauma Data Bank analysis. Ann Surg. 2011;253:371–377. - PubMed
-
- McSwain NE, Jr. Scott B. Frame, MD Memorial Lecture. Judgment based on knowledge: a history of Prehospital trauma life support, 1970–2013. J Trauma Acute Care Surg. 2013;75:1–7. - PubMed
-
- Taghavi S, Vora HP, Jayarajan SN, Gaughan JP, Pathak AS, Santora TA, Goldberg AJ. Prehospital intubation does not decrease complications in the penetrating trauma patient. Am Surg. 2014;80(1):9–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
