

Cardiac Resynchronization Therapy Response Assessment with Electromechanical Activation Mapping within 24 Hours of Device Implantation: A Pilot Study
- PMID: 33675941
- PMCID: PMC8263475
- DOI: 10.1016/j.echo.2021.02.012
Cardiac Resynchronization Therapy Response Assessment with Electromechanical Activation Mapping within 24 Hours of Device Implantation: A Pilot Study
Abstract
Background: Cardiac resynchronization therapy (CRT) response assessment relies on the QRS complex narrowing criterion. Yet one third of patients do not improve despite narrowed QRS after implantation. Electromechanical wave imaging (EWI) is a quantitative echocardiography-based technique capable of noninvasively mapping cardiac electromechanical activation in three dimensions. The aim of this exploratory study was to investigate the EWI technique, sensitive to ventricular dyssynchrony, for informing CRT response on the day of implantation.
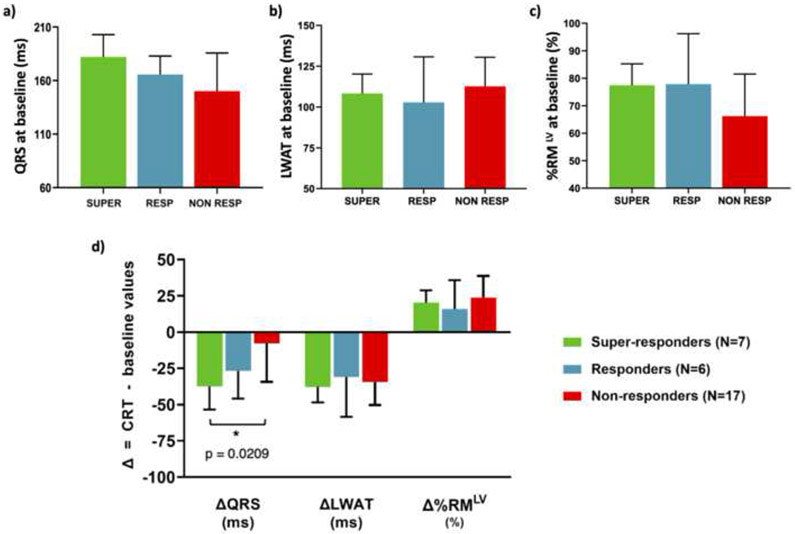
Methods: Forty-four patients with heart failure with left bundle branch block or right ventricular (RV) paced rhythm and decreased left ventricular ejection fraction (LVEF; mean, 25.3 ± 9.6%) underwent EWI without and with CRT within 24 hours of device implantation. Of those, 16 were also scanned while in left ventricular (LV) pacing. Improvement in LVEF at 3-, 6-, or 9-month follow-up defined (1) super-responders (ΔLVEF ≥ 20%), (2) responders (10% ≤ ΔLVEF < 20%), and (3) nonresponders (ΔLVEF ≤ 5%). Three-dimensionally rendered electromechanical maps were obtained under RV, LV, and biventricular CRT pacing conditions. Mean RV free wall and LV lateral wall activation times were computed. The percentage of resynchronized myocardium was measured by quantifying the percentage of the left ventricle activated within 120 msec of QRS onset. Correlations between percentage of resynchronized myocardium and type of CRT response were assessed.
Results: LV lateral wall activation time was significantly different (P ≤ .05) among all three pacing conditions in the 16 patients: LV lateral wall activation time with CRT in biventricular pacing (73.1 ± 17.6 msec) was lower compared with LV pacing (89.5 ± 21.5 msec) and RV pacing (120.3 ± 17.8 msec). Retrospective analysis showed that the percentage of resynchronized myocardium with CRT was a reliable response predictor within 24 hours of implantation for significantly (P ≤ .05) identifying super-responders (n = 7; 97.7 ± 1.9%) from nonresponders (n = 17; 89.9 ± 9.9%).
Conclusion: Electromechanical activation mapping constitutes a valuable three-dimensional visualization tool within 24 hours of implantation and could potentially aid in the timely assessment of CRT response rates, including during implantation for adjustment of lead placement and pacing outcomes.
Keywords: Cardiac resynchronization therapy; Echocardiography; Electromechanical wave imaging; Heart failure; Response prediction; Ventricular resynchrony assessment.
Copyright © 2021 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Figures





Similar articles
-
Cardiac resynchronization therapy in patients with heart failure and narrow QRS complexes (≤ 130 ms): role of speckle tracking echocardiography and different interventricular (VV) pacing intervals.J Interv Card Electrophysiol. 2022 Mar;63(2):369-377. doi: 10.1007/s10840-021-01021-y. Epub 2021 Jun 17. J Interv Card Electrophysiol. 2022. PMID: 34138397
-
Imaging the Propagation of the Electromechanical Wave in Heart Failure Patients with Cardiac Resynchronization Therapy.Pacing Clin Electrophysiol. 2017 Jan;40(1):35-45. doi: 10.1111/pace.12964. Epub 2016 Dec 2. Pacing Clin Electrophysiol. 2017. PMID: 27790723 Free PMC article. Review.
-
Cardiac resynchronization therapy with sequential biventricular pacing: impact of echocardiography guided VV delay optimization on acute results.Rev Port Cardiol. 2005 Nov;24(11):1355-65. Rev Port Cardiol. 2005. PMID: 16463985 English, Portuguese.
-
RV electrical activation in heart failure during right, left, and biventricular pacing.JACC Cardiovasc Imaging. 2010 Jun;3(6):567-75. doi: 10.1016/j.jcmg.2009.12.017. JACC Cardiovasc Imaging. 2010. PMID: 20541711 Free PMC article.
-
Assessment of mechanical dyssynchrony in cardiac resynchronization therapy.Dan Med J. 2014 Dec;61(12):B4981. Dan Med J. 2014. PMID: 25441737 Review.
Cited by
-
A New Electromechanical Wave Imaging Dispersion Metric for the Characterization of Ventricular Activation in Different Cardiac Resynchronization Therapy Pacing Schemes.IEEE Trans Biomed Eng. 2023 Mar;70(3):853-859. doi: 10.1109/TBME.2022.3203653. Epub 2023 Feb 17. IEEE Trans Biomed Eng. 2023. PMID: 36049009 Free PMC article.
-
High volume-rate echocardiography for simultaneous imaging of electromechanical activation and cardiac strain of the whole heart in a single heartbeat in humans.PLoS One. 2024 Dec 27;19(12):e0313410. doi: 10.1371/journal.pone.0313410. eCollection 2024. PLoS One. 2024. PMID: 39729494 Free PMC article.
References
-
- Gregoratos G, Abrams J, Epstein AE, Freedman RA, Hayes DL, Hlatky MA, et al. ACC/AHA/NASPE 2002 guideline update for implantation of cardiac pacemakers and antiarrhythmia devices—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/NASPE Committee to Update the 1998 Pacemaker Guidelines). J Am Coll Cardiol 2002; 40:1703–19. - PubMed
-
- Auricchio A, Prinzen FW. Non-responders to cardiac resynchronization therapy. Circ J 2011; 75:521–7. - PubMed
-
- Zareba W, Klein H, Cygankiewicz I, Hall WJ, McNitt S, Brown M, et al. Effectiveness of cardiac resynchronization therapy by qrs morphology in the Multicenter Automatic Defibrillator Implantation Trial–Cardiac Resynchronization Therapy (MADIT-CRT). Circulation 2011; 123:1061–72. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
