

A comprehensive assessment of environmental exposures and the medical history guides multidisciplinary discussion in interstitial lung disease
- PMID: 33676119
- PMCID: PMC7992253
- DOI: 10.1016/j.rmed.2021.106333
A comprehensive assessment of environmental exposures and the medical history guides multidisciplinary discussion in interstitial lung disease
Abstract
Background: Multidisciplinary discussion (MDD) is widely recommended for patients with interstitial lung disease (ILD), but published primary data from MDD has been scarce, and factors influencing MDD other than chest computed tomography (CT) and lung histopathology interpretations have not been well-described.
Methods: Single institution MDD of 179 patients with ILD.
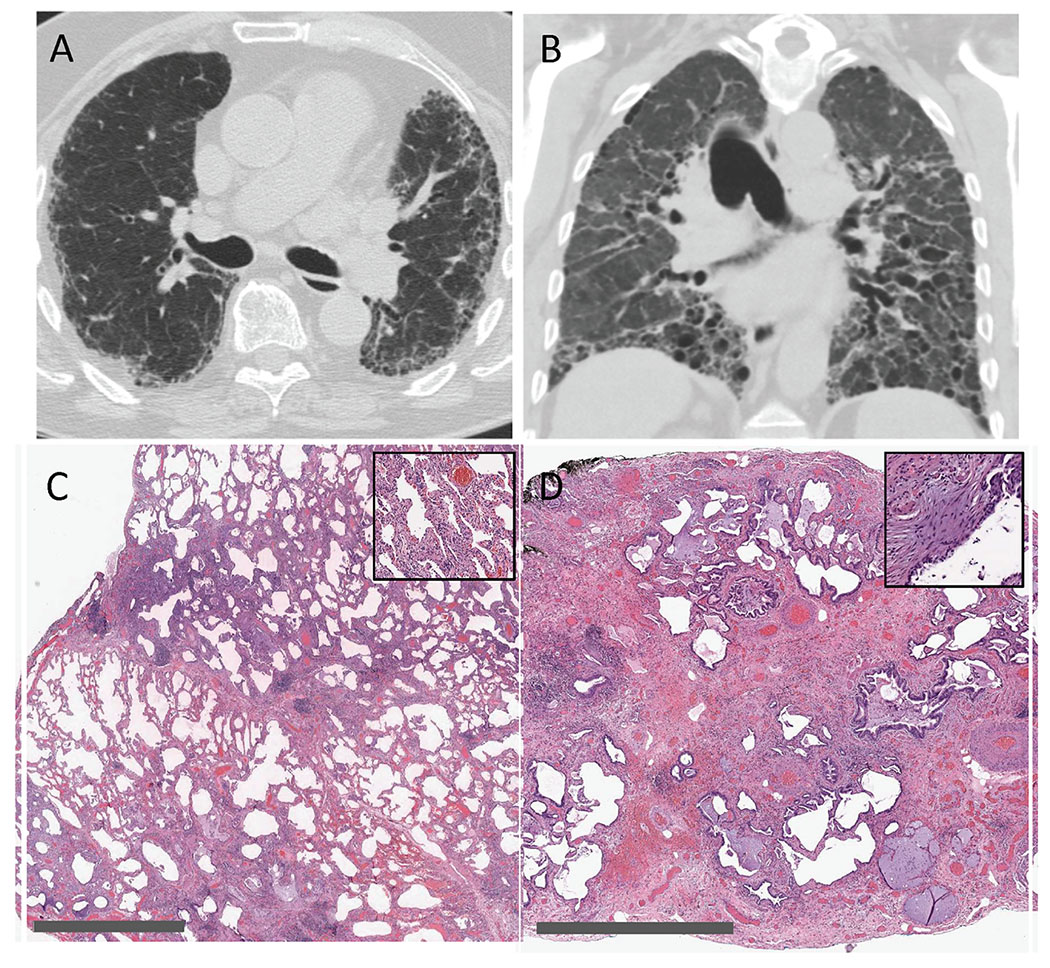
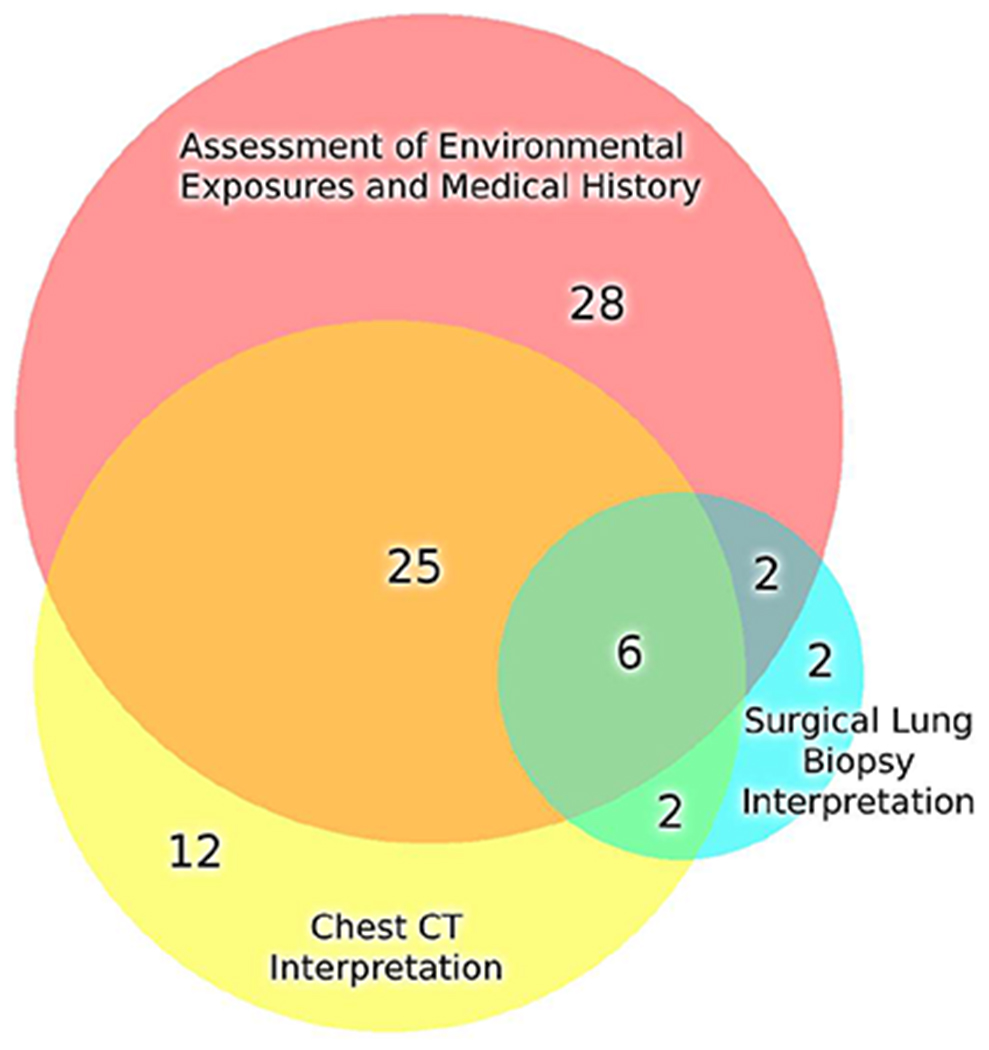
Results: MDD consensus clinical diagnoses included autoimmune-related ILD, chronic hypersensitivity pneumonitis, smoking-related ILD, idiopathic pulmonary fibrosis, medication-induced ILD, occupation-related ILD, unclassifiable ILD, and a few less common pulmonary disorders. In 168 of 179 patients, one or more environmental exposures or pertinent features of the medical history were identified, including recreational/avocational, residential, and occupational exposures, systemic autoimmune disease, malignancy, medication use, and family history. The MDD process demonstrated the importance of comprehensively assessing these exposures and features, beyond merely noting their presence, for rendering consensus clinical diagnoses. Precise, well-defined chest CT and lung histopathology interpretations were rendered at MDD, including usual interstitial pneumonia, nonspecific interstitial pneumonia, and organizing pneumonia, but these interpretations were associated with a variety of MDD consensus clinical diagnoses, demonstrating their nonspecific nature in many instances. In 77 patients in which MDD consensus diagnosis differed from referring diagnosis, assessment of environmental exposures and medical history was found retrospectively to be the most impactful factor.
Conclusions: A comprehensive assessment of environmental exposures and pertinent features of the medical history guided MDD. In addition to rendering consensus clinical diagnoses, MDD presented clinicians with opportunities to initiate environmental remediation, behavior modification, or medication alteration likely to benefit individual patients with ILD.
Keywords: Autoimmune; Hypersensitivity; Idiopathic pulmonary fibrosis; Interstitial lung disease; Multidisciplinary discussion; Occupation; Smoking.
Published by Elsevier Ltd.
Conflict of interest statement
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Demystifying idiopathic interstitial pneumonia: time for more etiology-focused nomenclature in interstitial lung disease.Expert Rev Respir Med. 2022 Feb;16(2):235-245. doi: 10.1080/17476348.2022.2030710. Epub 2022 Jan 31. Expert Rev Respir Med. 2022. PMID: 35034567 Free PMC article. Review.
-
[Chinese expert consensus on multidisciplinary discussion of interstitial lung disease].Zhonghua Jie He He Hu Xi Za Zhi. 2023 Dec 12;46(12):1176-1188. doi: 10.3760/cma.j.cn112147-20230726-00030. Zhonghua Jie He He Hu Xi Za Zhi. 2023. PMID: 37989522 Chinese.
-
The providing multidisciplinary ILD diagnoses (PROMISE) study - study design of the national registry of Japan facilitating interactive online multidisciplinary discussion diagnosis.BMC Pulm Med. 2024 Oct 14;24(1):511. doi: 10.1186/s12890-024-03232-1. BMC Pulm Med. 2024. PMID: 39396941 Free PMC article.
-
Sex-specific aspects in a population of patients undergoing evaluation for interstitial lung disease with transbronchial cryobiopsy.Sci Rep. 2025 Apr 5;15(1):11730. doi: 10.1038/s41598-025-94575-0. Sci Rep. 2025. PMID: 40188253 Free PMC article.
-
Identification and Remediation of Environmental Exposures in Patients With Interstitial Lung Disease: Evidence Review and Practical Considerations.Chest. 2021 Jul;160(1):219-230. doi: 10.1016/j.chest.2021.02.021. Epub 2021 Feb 18. Chest. 2021. PMID: 33609518 Free PMC article. Review.
Cited by
-
Demystifying idiopathic interstitial pneumonia: time for more etiology-focused nomenclature in interstitial lung disease.Expert Rev Respir Med. 2022 Feb;16(2):235-245. doi: 10.1080/17476348.2022.2030710. Epub 2022 Jan 31. Expert Rev Respir Med. 2022. PMID: 35034567 Free PMC article. Review.
-
Diagnostic yield and safety of transbronchial lung cryobiopsy using 1.7-mm probes in interstitial lung disease.J Thorac Dis. 2025 Jun 30;17(6):3962-3970. doi: 10.21037/jtd-2024-2160. Epub 2025 Jun 23. J Thorac Dis. 2025. PMID: 40688314 Free PMC article.
-
Treatment patterns and patient journey in progressive pulmonary fibrosis: a cross-sectional survey.Respir Res. 2024 Oct 9;25(1):364. doi: 10.1186/s12931-024-02995-9. Respir Res. 2024. PMID: 39385232 Free PMC article.
-
Occupational Lung Diseases: Spectrum of Common Imaging Manifestations.Korean J Radiol. 2023 Aug;24(8):795-806. doi: 10.3348/kjr.2023.0274. Korean J Radiol. 2023. PMID: 37500580 Free PMC article. Review.
-
Role of the occupational disease consultant in the multidisciplinary discussion of interstitial lung diseases.Respir Res. 2022 Dec 8;23(1):332. doi: 10.1186/s12931-022-02257-6. Respir Res. 2022. PMID: 36482462 Free PMC article.
References
-
- De Sadeleer LJ, Meert C, Yserbyt J, et al. Diagnostic Ability of a Dynamic Multidisciplinary Discussion in Interstitial Lung Diseases: A Retrospective Observational Study of 938 Cases. Chest. 2018;153(6):1416–1423. - PubMed
-
- Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2018;198(5):e44–e68. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
