

A standardized approach for exact CT-based three-dimensional position analysis in the distal tibiofibular joint
- PMID: 33676399
- PMCID: PMC7937306
- DOI: 10.1186/s12880-021-00570-y
A standardized approach for exact CT-based three-dimensional position analysis in the distal tibiofibular joint
Abstract
Background: Assessment of tibiofibular reduction presents an intra- and postoperative challenge. Numerous two-dimensional measurement methods have been described, most of them highly dependent on leg orientation and rater. Aim of the present work was to develop a standardized and orientation-independent 3D based method for the assessment of syndesmotic joint position.
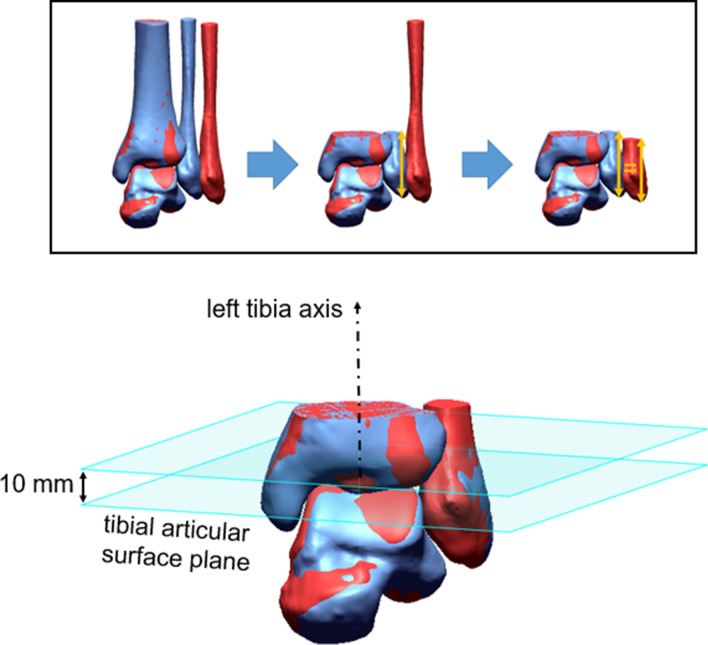
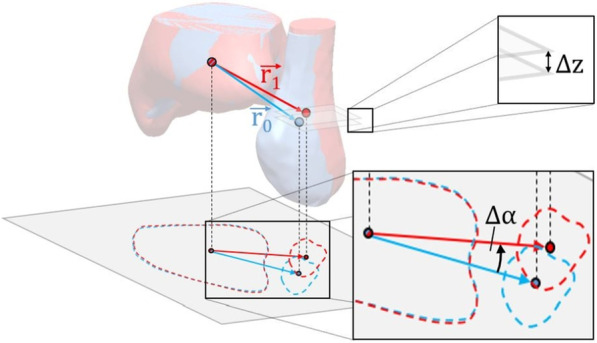
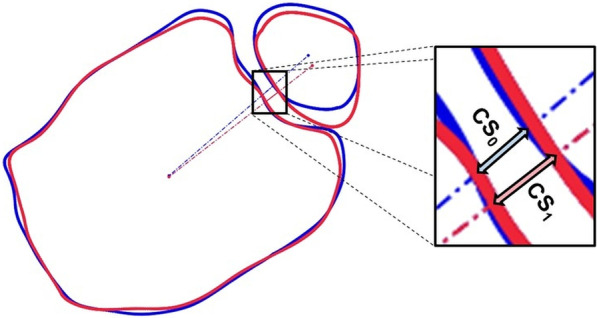
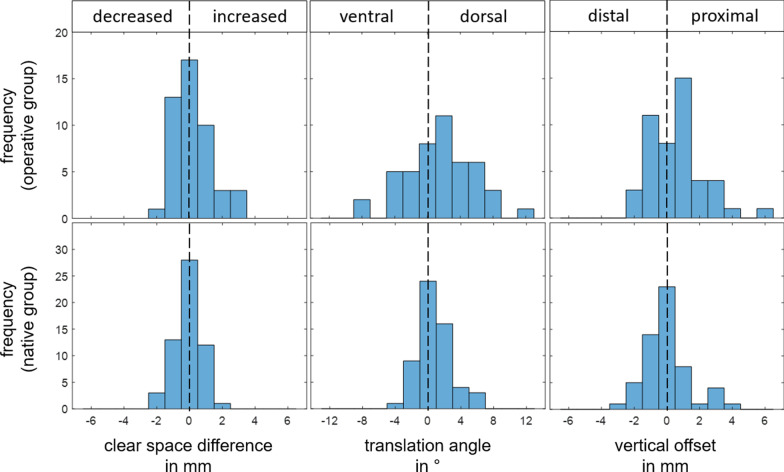
Methods: In a retrospective single center study, 3D models of bilateral ankle joints, either after unilateral syndesmosis stabilization (operative group) or with no injury (native group) were superimposed (best fit matching) and aligned uniformly. Based on center of gravity calculations three orientation- and rater-independent parameters were determined: tibiofibular clears space (CS), vertical offset between both fibulae, and translation angle of the fibulae about tibia axis.
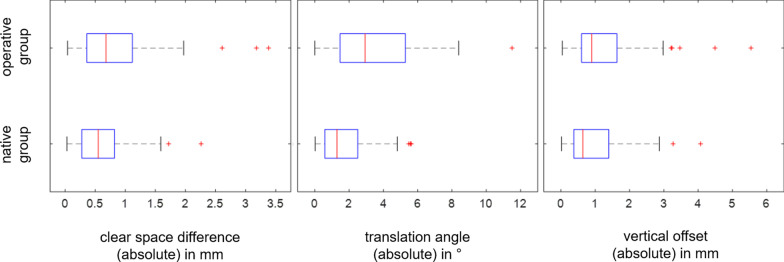
Results: Bilateral CT datasets of 57 native and 47 postoperative patients were analyzed. In the native group mean CS was 2.7 (SD, 0.8; range, 0.7-4.9) mm, mean CS side difference was 0.62 (SD, 0.45) mm and mean translation angle was 1.6 (SD, 1.4) degrees regarding absolute values. The operative group was found to show a significantly higher CS side difference of 0.88 (SD, 0.75) mm compared to native group (P = .046). Compared to the healthy contralateral side, operated fibulae showed mean proximal displacement of 0.56 (SD, 1.67) mm (P = .025), dorsal displacement of 1.5 (SD 4.1) degrees (P = .017).
Conclusion: By using 3D best fit matching, orientation- and rater-dependent errors can be minimized. Large interindividual and small intraindividual differences of uninjured couples support previous recommendations for bilateral imaging.
Trial registration: AZ 131/18-ek; AZ 361/19-ek LEVEL OF EVIDENCE: Level III.
Keywords: 3D Position control; Ankle; CT; Clear space; Syndesmosis; Tibiofibular.
Conflict of interest statement
The authors declare no conflict of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Purvis GD. Displaced, unstable ankle fractures: classification, incidence, and management of a consecutive series. Clinical orthopaedics and related research. 1982;:91–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
