

Risk of adverse outcomes in patients with underlying respiratory conditions admitted to hospital with COVID-19: a national, multicentre prospective cohort study using the ISARIC WHO Clinical Characterisation Protocol UK
- PMID: 33676593
- PMCID: PMC8241313
- DOI: 10.1016/S2213-2600(21)00013-8
Risk of adverse outcomes in patients with underlying respiratory conditions admitted to hospital with COVID-19: a national, multicentre prospective cohort study using the ISARIC WHO Clinical Characterisation Protocol UK
Abstract
Background: Studies of patients admitted to hospital with COVID-19 have found varying mortality outcomes associated with underlying respiratory conditions and inhaled corticosteroid use. Using data from a national, multicentre, prospective cohort, we aimed to characterise people with COVID-19 admitted to hospital with underlying respiratory disease, assess the level of care received, measure in-hospital mortality, and examine the effect of inhaled corticosteroid use.
Methods: We analysed data from the International Severe Acute Respiratory and emerging Infection Consortium (ISARIC) WHO Clinical Characterisation Protocol UK (CCP-UK) study. All patients admitted to hospital with COVID-19 across England, Scotland, and Wales between Jan 17 and Aug 3, 2020, were eligible for inclusion in this analysis. Patients with asthma, chronic pulmonary disease, or both, were identified and stratified by age (<16 years, 16-49 years, and ≥50 years). In-hospital mortality was measured by use of multilevel Cox proportional hazards, adjusting for demographics, comorbidities, and medications (inhaled corticosteroids, short-acting β-agonists [SABAs], and long-acting β-agonists [LABAs]). Patients with asthma who were taking an inhaled corticosteroid plus LABA plus another maintenance asthma medication were considered to have severe asthma.
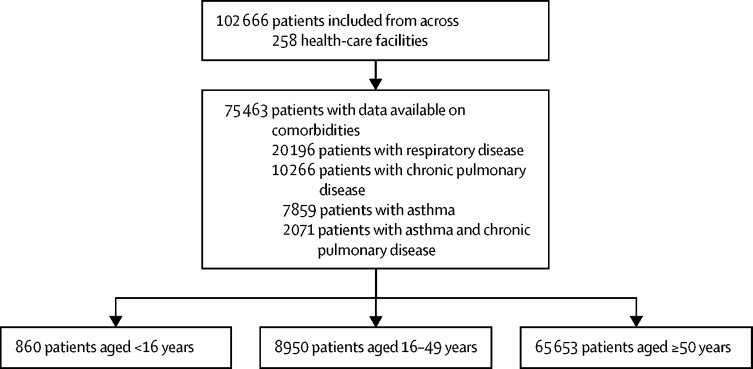
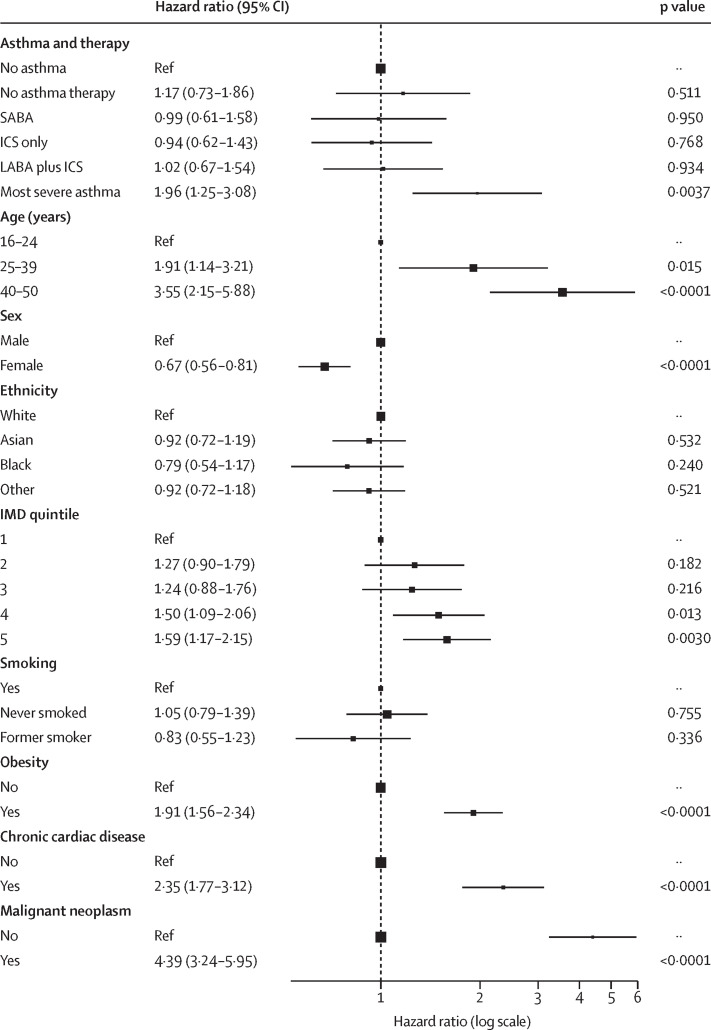
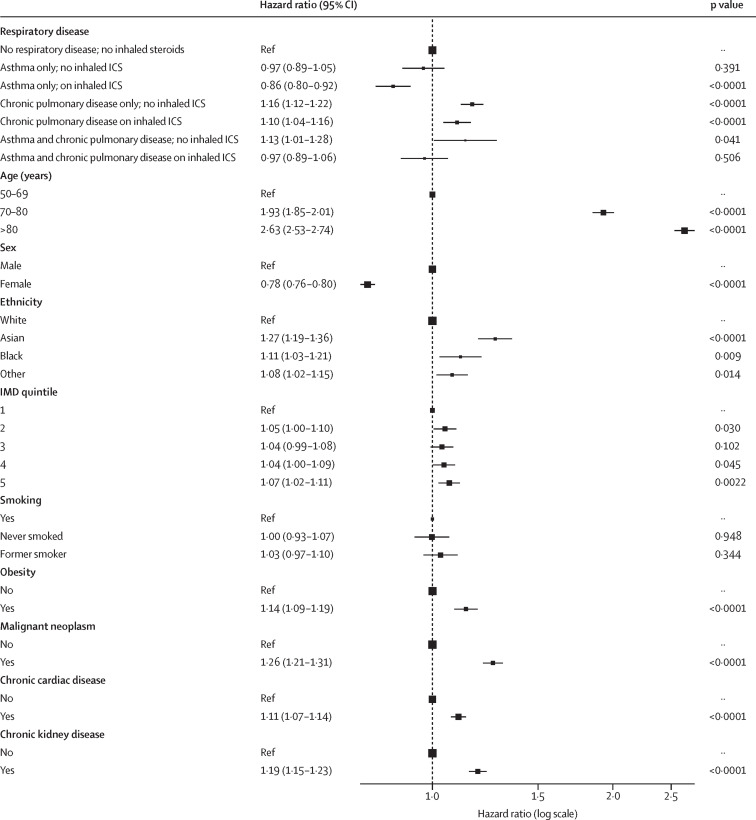
Findings: 75 463 patients from 258 participating health-care facilities were included in this analysis: 860 patients younger than 16 years (74 [8·6%] with asthma), 8950 patients aged 16-49 years (1867 [20·9%] with asthma), and 65 653 patients aged 50 years and older (5918 [9·0%] with asthma, 10 266 [15·6%] with chronic pulmonary disease, and 2071 [3·2%] with both asthma and chronic pulmonary disease). Patients with asthma were significantly more likely than those without asthma to receive critical care (patients aged 16-49 years: adjusted odds ratio [OR] 1·20 [95% CI 1·05-1·37]; p=0·0080; patients aged ≥50 years: adjusted OR 1·17 [1·08-1·27]; p<0·0001), and patients aged 50 years and older with chronic pulmonary disease (with or without asthma) were significantly less likely than those without a respiratory condition to receive critical care (adjusted OR 0·66 [0·60-0·72] for those without asthma and 0·74 [0·62-0·87] for those with asthma; p<0·0001 for both). In patients aged 16-49 years, only those with severe asthma had a significant increase in mortality compared to those with no asthma (adjusted hazard ratio [HR] 1·17 [95% CI 0·73-1·86] for those on no asthma therapy, 0·99 [0·61-1·58] for those on SABAs only, 0·94 [0·62-1·43] for those on inhaled corticosteroids only, 1·02 [0·67-1·54] for those on inhaled corticosteroids plus LABAs, and 1·96 [1·25-3·08] for those with severe asthma). Among patients aged 50 years and older, those with chronic pulmonary disease had a significantly increased mortality risk, regardless of inhaled corticosteroid use, compared to patients without an underlying respiratory condition (adjusted HR 1·16 [95% CI 1·12-1·22] for those not on inhaled corticosteroids, and 1·10 [1·04-1·16] for those on inhaled corticosteroids; p<0·0001). Patients aged 50 years and older with severe asthma also had an increased mortality risk compared to those not on asthma therapy (adjusted HR 1·24 [95% CI 1·04-1·49]). In patients aged 50 years and older, inhaled corticosteroid use within 2 weeks of hospital admission was associated with decreased mortality in those with asthma, compared to those without an underlying respiratory condition (adjusted HR 0·86 [95% CI 0·80-0·92]).
Interpretation: Underlying respiratory conditions are common in patients admitted to hospital with COVID-19. Regardless of the severity of symptoms at admission and comorbidities, patients with asthma were more likely, and those with chronic pulmonary disease less likely, to receive critical care than patients without an underlying respiratory condition. In patients aged 16 years and older, severe asthma was associated with increased mortality compared to non-severe asthma. In patients aged 50 years and older, inhaled corticosteroid use in those with asthma was associated with lower mortality than in patients without an underlying respiratory condition; patients with chronic pulmonary disease had significantly increased mortality compared to those with no underlying respiratory condition, regardless of inhaled corticosteroid use. Our results suggest that the use of inhaled corticosteroids, within 2 weeks of admission, improves survival for patients aged 50 years and older with asthma, but not for those with chronic pulmonary disease.
Funding: National Institute for Health Research, Medical Research Council, NIHR Health Protection Research Units in Emerging and Zoonotic Infections at the University of Liverpool and in Respiratory Infections at Imperial College London in partnership with Public Health England.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
References
-
- NHS Who's at higher risk from coronavirus. 2020. https://www.nhs.uk/conditions/coronavirus-covid-19/people-at-higher-risk...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
