

Diagnosis of non-consensus transient ischaemic attacks with focal, negative, and non-progressive symptoms: population-based validation by investigation and prognosis
- PMID: 33676629
- PMCID: PMC7938377
- DOI: 10.1016/S0140-6736(20)31961-9
Diagnosis of non-consensus transient ischaemic attacks with focal, negative, and non-progressive symptoms: population-based validation by investigation and prognosis
Abstract
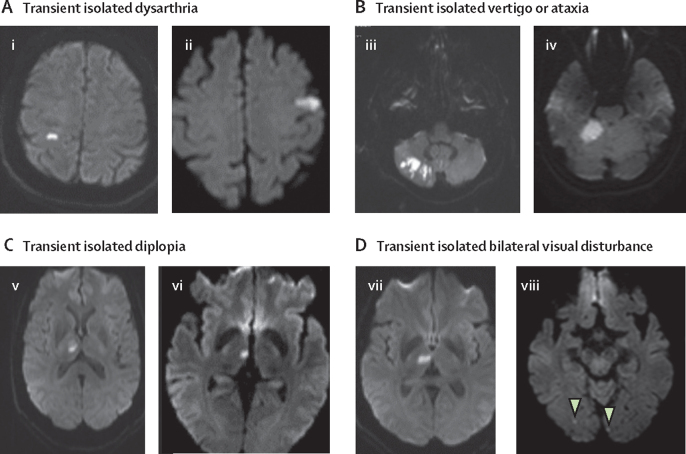
Background: Diagnosis of transient ischaemic attacks (TIAs) can be difficult. There is consensus on classic symptoms (eg, motor weakness, dysphasia, hemianopia, monocular visual loss) but no consensus on several monosymptomatic events with sudden-onset, non-progressive, focal negative symptoms (eg, isolated diplopia, dysarthria, vertigo, ataxia, sensory loss, and bilateral visual disturbance), with much variation in investigation and treatment.
Methods: We prospectively ascertained and investigated all strokes and sudden onset transient neurological symptoms in a population of 92 728 people (no age restrictions) from Oxfordshire, UK, who sought medical attention at nine primary care practices or at the John Radcliffe Hospital, Oxford, UK (Oxford Vascular Study). Patients classified at baseline with minor ischaemic stroke (National Institutes of Health Stroke Score <5), classic TIA, or non-consensus TIA were treated according to secondary prevention guidelines. Risks of stroke (7-day, 90-day, and 10-year risks) and risks of all major vascular events (from the time of first event, and from the time of seeking medical attention) were established by face-to-face follow-up visits and were compared with the risk expected from age and sex-specific stroke incidence in the underlying study population.
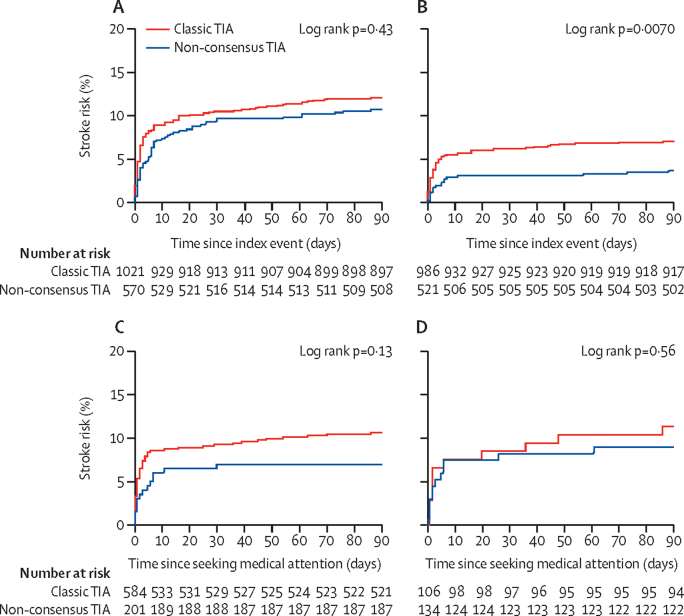
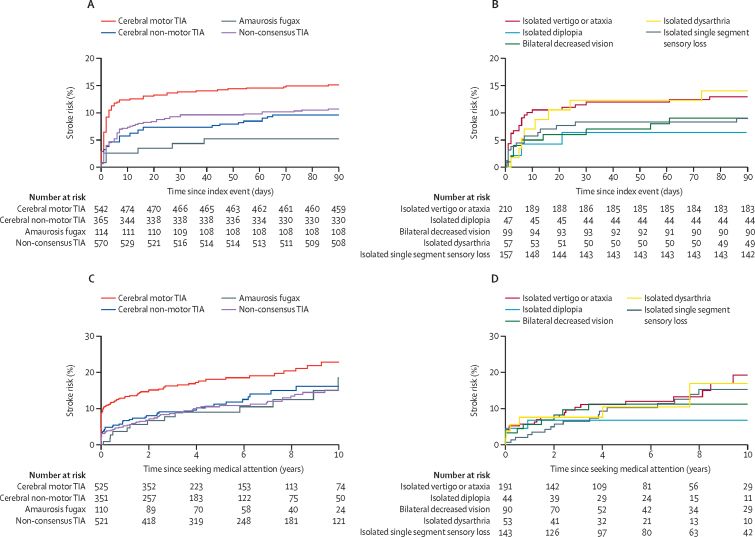
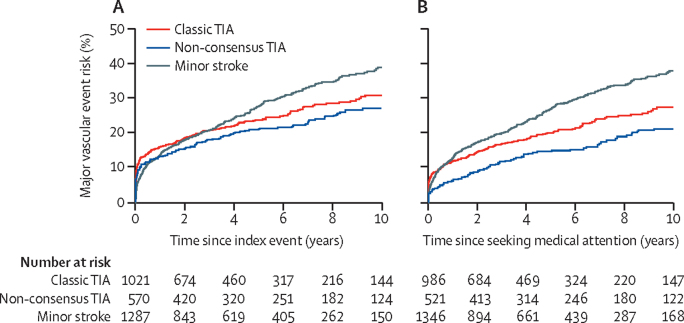
Findings: Between April 1, 2002, and March 31, 2018, 2878 patients were identified with minor ischaemic stroke (n=1287), classic TIA (n=1021), or non-consensus TIA (n=570). Follow-up was to Oct 1, 2018 (median 5·2 [IQR 2·6-9·2] years). 577 first recurrent strokes after the index event occurred during 17 009 person-years of follow-up. 90-day stroke risk from time of the index event after a non-consensus TIA was similar to that after classic TIA (10·6% [95% CI 7·8-12·9] vs 11·6% [95% CI 9·6-13·6]; hazard ratio 0·87, 95% CI 0·64-1·19; p=0·43), and higher than after amaurosis fugax (4·3% [95% CI 0·6-8·0]; p=0·042). However, patients with non-consensus TIA were less likely to seek medical attention on the day of the event than were those with classic TIA (336 of 570 [59%] vs 768 of 1021 [75%]; odds ratio [OR] 0·47, 95% CI 0·38-0·59; p<0·0001) and were more likely to have recurrent strokes before seeking attention (45 of 570 [8%] vs 47 of 1021 [5%]; OR 1·77, 95% CI 1·16-2·71; p=0·007). After excluding such recurrent strokes, 7-day stroke risk after seeking attention for non-consensus TIA (2·9% [95% CI 1·5-4·3]) was still considerably higher than the expected background risk (relative risk [RR] 203, 95% CI 113-334), particularly if the patient sought attention on the day of the index event (5·0% [2·1-7·9]; RR 300, 137-569). 10-year risk of all major vascular events was similar for non-consensus and classic TIAs (27·1% [95% CI 22·8-31·4] vs 30·9% [27·2-33·7]; p=0·12). Baseline prevalence of atrial fibrillation, patent foramen ovale, and arterial stenoses were also similar for non-consensus TIA and classic TIA, although stenoses in the posterior circulation were more frequent with non-consensus TIA (OR 2·21, 95% CI 1·59-3·08; p<0·0001).
Interpretation: Patients with non-consensus TIA are at high early and long-term risk of stroke and have cardiovascular pathological findings on investigation similar to those of classic TIA. Designation of non-consensus TIAs as definite cerebrovascular events will increase overall TIA diagnoses by about 50%.
Funding: Wellcome Trust, National Institute for Health Research Oxford Biomedical Research Centre, Wolfson Foundation, Masonic Charitable Foundation, and British Heart Foundation.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Im Zweifel ist es doch eine TIA.MMW Fortschr Med. 2021 Jun;163(12):24-25. doi: 10.1007/s15006-021-0036-z. MMW Fortschr Med. 2021. PMID: 34146272 Review. German. No abstract available.
References
-
- Giles MF, Rothwell PM. Risk of stroke early after transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol. 2007;6:1063–1072. - PubMed
-
- Johnston SC, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901–2906. - PubMed
-
- Rothwell PM, Giles MF, Chandratheva A. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370:1432–1442. - PubMed
-
- Lavallee PC, Meseguer E, Abboud H. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6:953–960. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
