

Transpulmonary pressure measurements and lung mechanics in patients with early ARDS and SARS-CoV-2
- PMID: 33676795
- PMCID: PMC7906505
- DOI: 10.1016/j.jcrc.2021.02.005
Transpulmonary pressure measurements and lung mechanics in patients with early ARDS and SARS-CoV-2
Abstract
Purpose: Acute Respiratory Distress Syndrome (ARDS) secondary to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has demonstrated variable oxygenation and respiratory-system mechanics without investigation of transpulmonary and chest-wall mechanics. This study describes lung, chest wall and respiratory-system mechanics in patients with SARS-CoV-2 and ARDS.
Methods: Data was collected from forty patients with confirmed SARS-CoV-2 and ARDS at Beth Israel Deaconess Medical Center in Boston, Massachusetts. Esophageal balloons were placed to estimate pleural and transpulmonary pressures. Clinical characteristics, respiratory-system, transpulmonary, and chest-wall mechanics were measured over the first week.
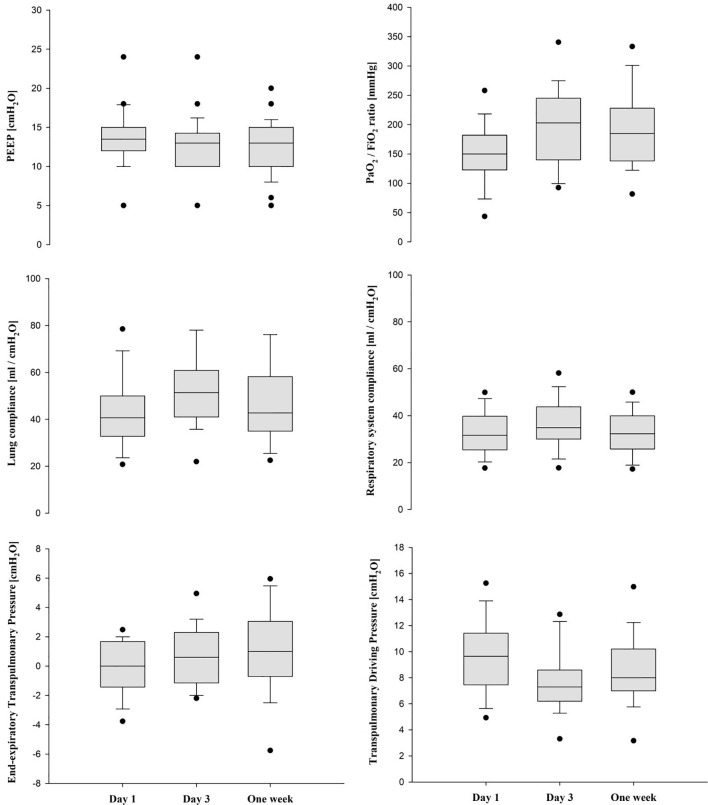
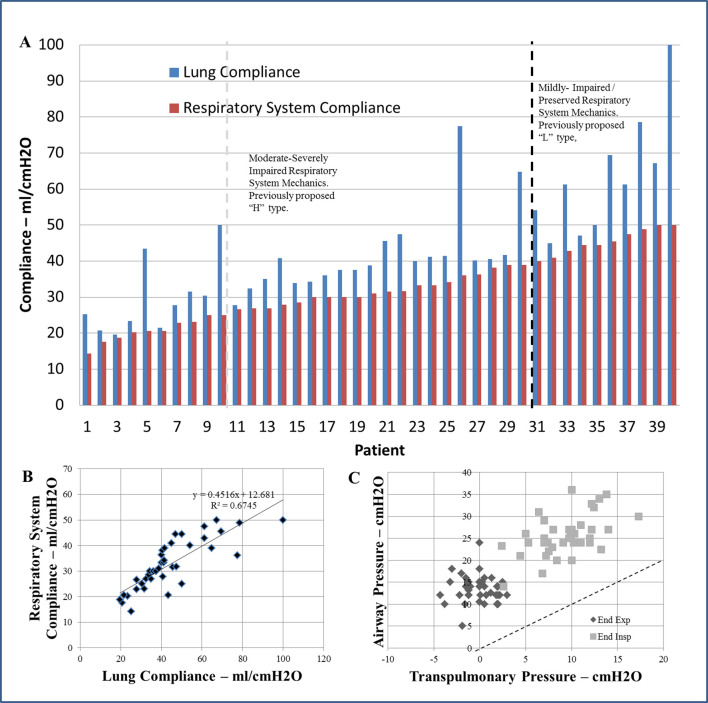
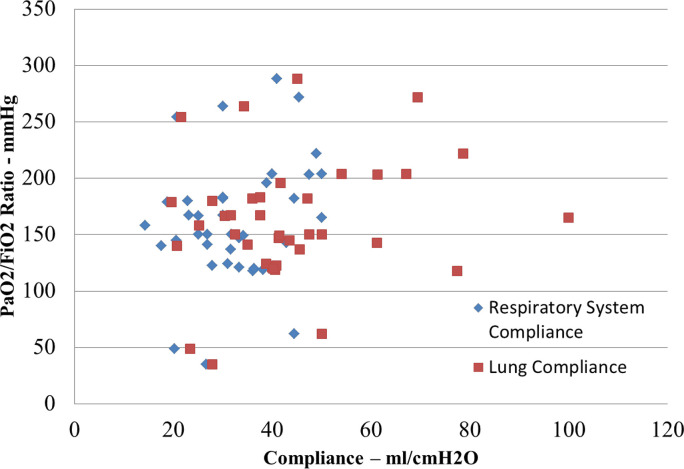
Results: Patients had moderate-severe ARDS (PaO2/FiO2 123[98-149]) and were critically ill (APACHE IV 108 [94-128] and SOFA 12 [11-13]). PaO2/FiO2 improved over the first week (150 mmHg [122.9-182] to 185 mmHg [138-228] (p = 0.035)). Respiratory system (30-35 ml/cm H2O), lung (40-50 ml/cm H2O) and chest wall (120-150 ml/cm H2O) compliance remained similar over the first week. Elevated basal pleural pressures correlated with BMI. Patients required prolonged mechanical ventilation (14.5 days [9.5-19.0]), with a mortality of 32.5%.
Conclusions: Patients displayed normal chest-wall mechanics, with increased basal pleural pressure. Respiratory system and lung mechanics were similar to known existing ARDS cohorts. The wide range of respiratory system mechanics illustrates the inherent heterogeneity that is consistent with typical ARDS.
Keywords: ARDS; Acute respiratory distress syndrome; COVID-19; Chest wall mechanics; Coronavirus; Mechanical ventilation; Mechanics; SARS-CoV-2; Transpulmonary pressure.
Copyright © 2018. Published by Elsevier Inc.
Conflict of interest statement
Declaration of Competing Interest Dr. Baedorf Kassis and Dr. Talmor have received speaking fees for educational conferences from Hamilton Medical Inc. There are no conflicts related to the submitted research manuscript. As above, this work was conducted under the support of the NIHKL2 TR002542 award.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
