

Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort
- PMID: 33676998
- PMCID: PMC7930807
- DOI: 10.1016/j.chest.2021.02.062
Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort
Abstract
Background: More than 20% of hospitalized patients with COVID-19 demonstrate ARDS requiring ICU admission. The long-term respiratory sequelae in such patients remain unclear.
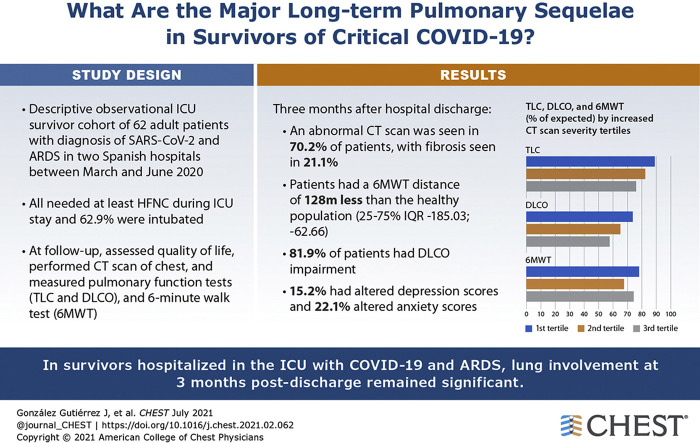
Research question: What are the major long-term pulmonary sequelae in critical patients who survive COVID-19?
Study design and methods: Consecutive patients with COVID-19 requiring ICU admission were recruited and evaluated 3 months after hospitalization discharge. The follow-up comprised symptom and quality of life, anxiety and depression questionnaires, pulmonary function tests, exercise test (6-min walking test [6MWT]), and chest CT imaging.
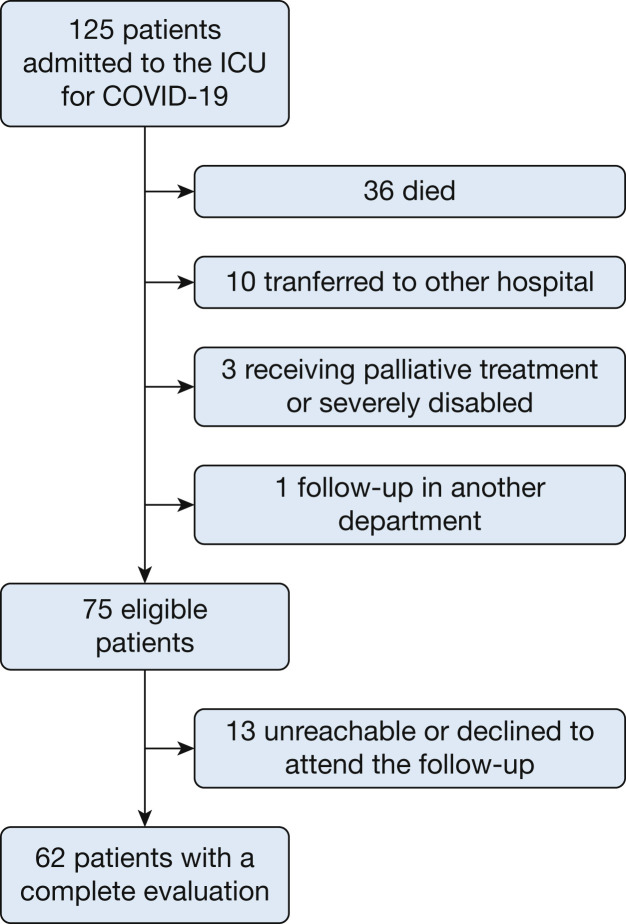
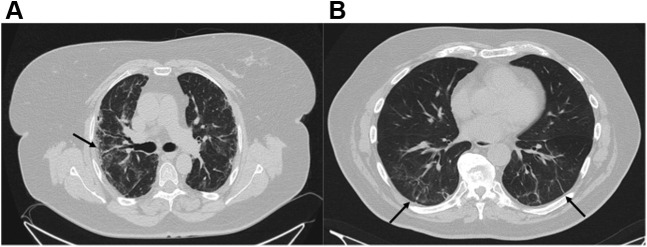
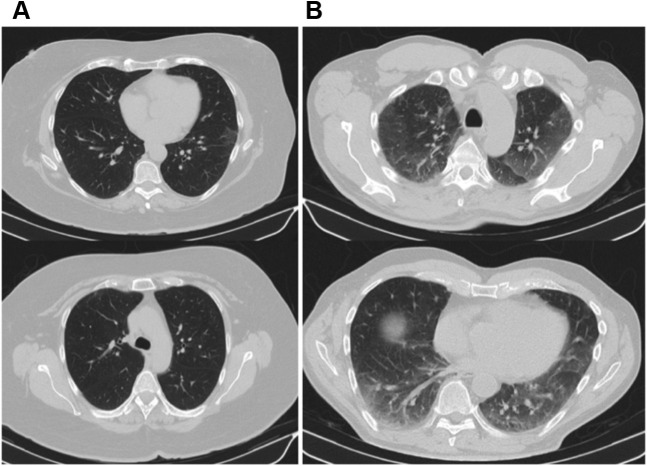
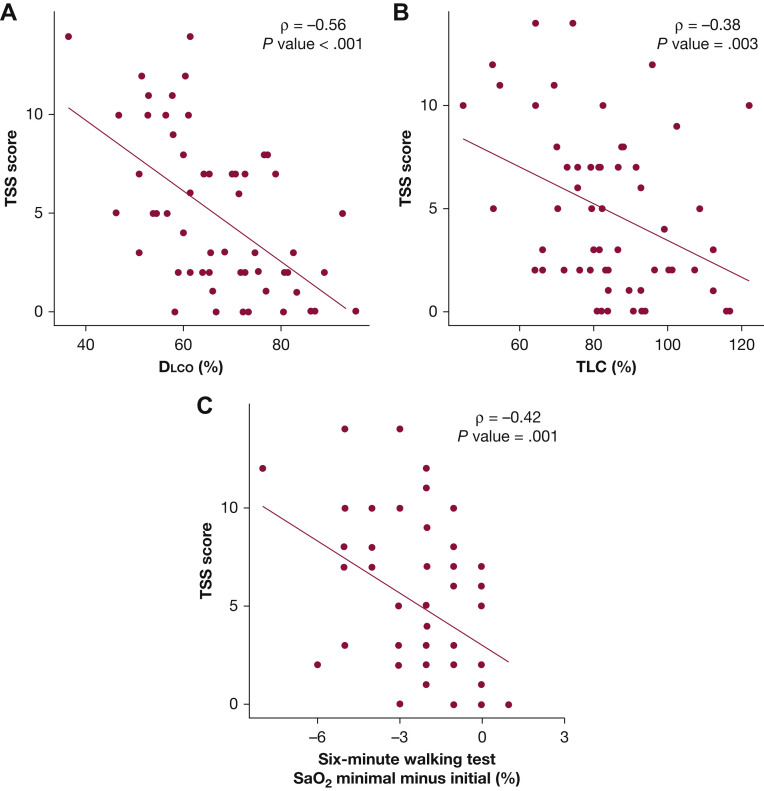
Results: One hundred twenty-five patients admitted to the ICU with ARDS secondary to COVID-19 were recruited between March and June 2020. At the 3-month follow-up, 62 patients were available for pulmonary evaluation. The most frequent symptoms were dyspnea (46.7%) and cough (34.4%). Eighty-two percent of patients showed a lung diffusing capacity of less than 80%. The median distance in the 6MWT was 400 m (interquartile range, 362-440 m). CT scans showed abnormal results in 70.2% of patients, demonstrating reticular lesions in 49.1% and fibrotic patterns in 21.1%. Patients with more severe alterations on chest CT scan showed worse pulmonary function and presented more degrees of desaturation in the 6MWT. Factors associated with the severity of lung damage on chest CT scan were age and length of invasive mechanical ventilation during the ICU stay.
Interpretation: Three months after hospital discharge, pulmonary structural abnormalities and functional impairment are highly prevalent in patients with ARDS secondary to COVID-19 who required an ICU stay. Pulmonary evaluation should be considered for all critical COVID-19 survivors 3 months after discharge.
Keywords: COVID-19; CT abnormalities; ICU; SARS; SARS-CoV-2; lung function; sequelae.
Copyright © 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Surviving COVID-19: A Burden Yet to Come?Chest. 2021 Jul;160(1):15-16. doi: 10.1016/j.chest.2021.04.019. Chest. 2021. PMID: 34246363 Free PMC article. No abstract available.
-
Residual Lung Defects Among Survivors of Severe COVID-19 Infection.Chest. 2022 Feb;161(2):e134. doi: 10.1016/j.chest.2021.09.034. Chest. 2022. PMID: 35131072 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
