

Beyond ratios - flexible and resilient nurse staffing options to deliver cost-effective hospital care and address staff shortages: A simulation and economic modelling study
- PMID: 33677251
- PMCID: PMC8220646
- DOI: 10.1016/j.ijnurstu.2021.103901
Beyond ratios - flexible and resilient nurse staffing options to deliver cost-effective hospital care and address staff shortages: A simulation and economic modelling study
Abstract
Background: In the face of pressure to contain costs and make best use of scarce nurses, flexible staff deployment (floating staff between units and temporary hires) guided by a patient classification system may appear an efficient approach to meeting variable demand for care in hospitals.
Objectives: We modelled the cost-effectiveness of different approaches to planning baseline numbers of nurses to roster on general medical/surgical units while using flexible staff to respond to fluctuating demand.
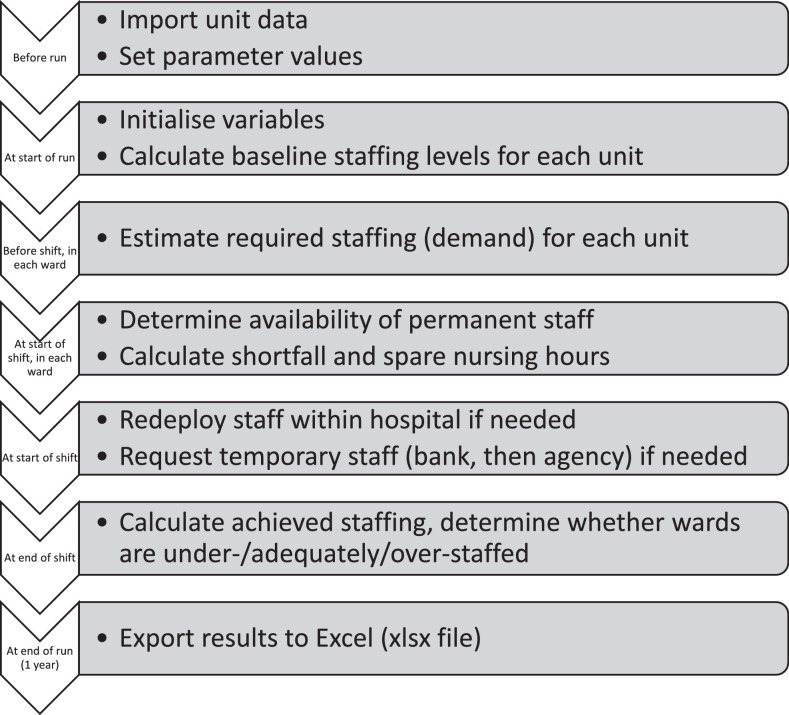
Design and setting: We developed an agent-based simulation, where hospital inpatient units move between being understaffed, adequately staffed or overstaffed as staff supply and demand (as measured by the Safer Nursing Care Tool patient classification system) varies. Staffing shortfalls are addressed by floating staff from overstaffed units or hiring temporary staff. We compared a standard staffing plan (baseline rosters set to match average demand) with a higher baseline 'resilient' plan set to match higher than average demand, and a low baseline 'flexible' plan. We varied assumptions about temporary staff availability and estimated the effect of unresolved low staffing on length of stay and death, calculating cost per life saved.
Results: Staffing plans with higher baseline rosters led to higher costs but improved outcomes. Cost savings from lower baseline staff mainly arose because shifts were left understaffed and much of the staff cost saving was offset by costs from longer patient stays. With limited temporary staff available, changing from low baseline flexible plan to the standard plan cost £13,117 per life saved and changing from the standard plan to the higher baseline 'resilient' plan cost £8,653 per life saved. Although adverse outcomes from low baseline staffing reduced when more temporary staff were available, higher baselines were even more cost-effective because the saving on staff costs also reduced. With unlimited temporary staff, changing from low baseline plan to the standard cost £4,520 per life saved and changing from the standard plan to the higher baseline cost £3,693 per life saved.
Conclusion: Shift-by-shift measurement of patient demand can guide flexible staff deployment, but the baseline number of staff rostered must be sufficient. Higher baseline rosters are more resilient in the face of variation and appear cost-effective. Staffing plans that minimise the number of nurses rostered in advance are likely to harm patients because temporary staff may not be available at short notice. Such plans, which rely heavily on flexible deployments, do not represent an efficient or effective use of nurses.
Study registration: ISRCTN 12307968 Tweetable abstract: Economic simulation model of hospital units shows low baseline staff levels with high use of flexible staff are not cost-effective and don't solve nursing shortages.
Keywords: Computer simulation; Cost savings; Costs and cost analysis; Health care economics and organizations; Hospital; Hospital information systems; Nursing administration research; Nursing staff; Operations research; Patient classification systems; Patient safety; Personnel staffing and scheduling; Quality of health care; Safer Nursing Care Tool; Workload.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest PG is a member of the National Health Service Improvement (NHSI) safe staffing faculty steering group. The safe staffing faculty programme is intended to ensure that knowledge of the Safer Nursing Care Tool (SNCT), its development and its operational application is consistently applied across the NHS.
Figures
References
-
- Bae S.H., Brewer C.S., Kelly M., Spencer A. Use of temporary nursing staff and nosocomial infections in intensive care units. J. Clin. Nurs. 2015;24(7–8):980–990. - PubMed
-
- Ball J., Barker H., Griffiths P., Jones J., Lawless J., Burton C.R., Couch R., Rycroft-Malone J. Report to Funders:. University of Southampton; Southampton: 2019. Implementation, Impact and Costs of Policies for Safe Staffing In Acute Trusts.
-
- Berg S.H., Akerjordet K., Ekstedt M., Aase K. Methodological strategies in resilient health care studies: an integrative review. Saf. Sci. 2018;110:300–312. doi: 10.1016/j.ssci.2018.08.025. - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
